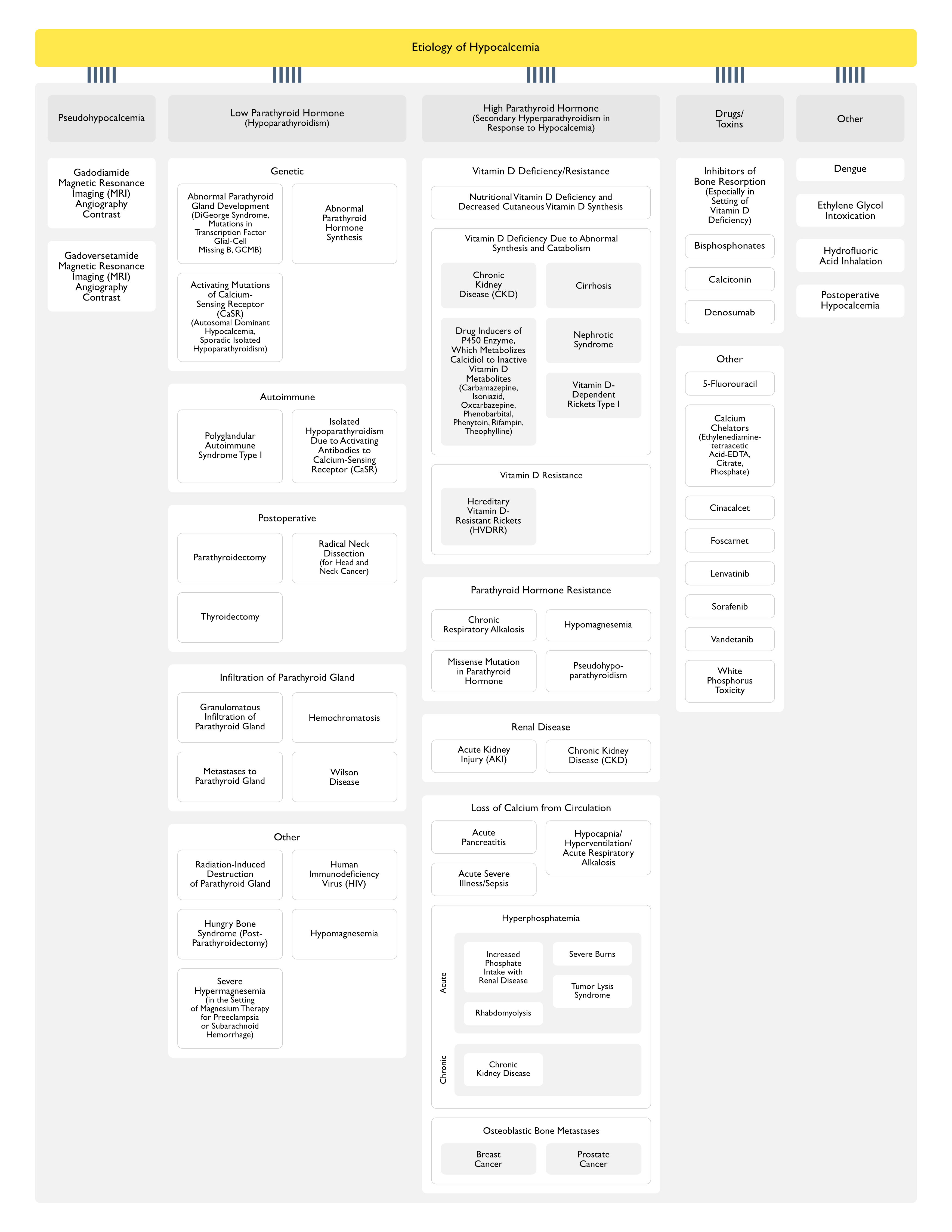
Mutations in the Transcription Factor Glial-Cell Missing B (GCMB)
Abnormal Parathyroid Hormone (PTH) Synthesis
Activating Mutations of Calcium-Sensing Receptor (CaSR)
Physiology
Activating Mutations of Calcium-Sensing Receptor (CaSR) Decrease the Set-Point of CaSR, So that Parathyroid Hormone (PTH) is Not Released at Serum Calcium Concentrations Which Would Normally Trigger Parathyroid Hormone (PTH) Release
Etiology
Autosomal Dominant Hypocalcemia
Sporadic Isolated Hypoparathyroidism
Diagnosis
Normal/High Urinary Calcium (Due to Increased Activation of CaSR in the Kidney)
Autoimmune
General Comments
Acquired Hypoparathyroidism Unrelated to Surgery is Most Commonly Due to Autoimmune Disease (Clin Exp Immunol, 1966) [MEDLINE] (Medicine-Baltimore, 1981) [MEDLINE]
Isolated Hypoparathyroidism Due to Activating Antibodies to Calcium-Sensing Receptor (CaSR)
Postoperative
General Comments
Surgical Etiologies are the Most Common Causes of Hypoparathyroidism
Postoperative Hypoparathyroidism Can Be Trasient (with Recovery in Days-Months), Intermittent, or Permanent
Transient Hypoparathyroidism May Be Due to Manipulation of the Blood Supply to the Parathyroid Gland or Removal or One or More of the Parathyroid Glands
Intermittent Hypoparathyroidism May Be Due to Decreased Parathyroid Reserve
Post-Parathyroidectomy Hypoparathyroidism May Be Transient (Due to Suppression of the Remaining Parathyroid Tissue by Prior Hypercalcemia) or May Be Severe/Prolonged (in Cases of Hungry Bone Syndrome)
Transient Hypoparathyroidism Occurs in Up to 20% of Patients After Surgery for Thyroid Cancer
Permanent Hypoparathyroidism Occurs in 0.8-3% of Patients After Total Thyroidectomy (Especially When the Goiter is Extensive and Anatomical Landmarks are Obscured)
Most Commonly Associated with Metastases (Typically in the Setting of Widely Metastatic Disease) from Breast Cancer, Lung Cancer, and Melanoma (Head Neck Pathol, 2018) [MEDLINE]
Occurs in the Setting o Serum Magnesium Concentration >5 mEq/L (>6 mg/dL, >2.5 mmol/L)
These Levels May Be Seen in the Setting of Magnesium Therapy for the Treatment of Preeclampsia (see Preeclampsia/Eclampsia)
These Levels May Be Seen in the Setting of Magnesium Therapy for the Treatment of Subarachnoid Hemorrhage (SAH) (see Subarachnoid Hemorrhage) (Neurocrit Care, 2008) [MEDLINE]
Physiology
Suppression of Parathyroid Hormone (PTH) Secretion (NEJM, 1984) [MEDLINE]
Clinical
Clinically Symptomatic Hypocalcemia Rarely Occurs, Due to the Presumably Short Duration of Hypermagnesemia and the Antagonistic Neuromuscular Effects of Hypermagnesemia
High Parathyroid Hormone (Secondary Hyperparathyroidism in Response to Hypocalcemia) (see Hyperparathyroidism)
Low Calcitriol (1,25 Dihydroxyvitamin D) Production Due to Decreased Glomerular Filtration Rate, Loss of the 1-Alpha-Hydroxylase Enzyme Secondary to Structural Renal Disease, and Suppression of Enzyme Activity Due to Hyperphosphatemia and Resultant Increased Circulating FGF23 Levels
Drugs (Inducers of P450 Enzyme, Which Metabolizes Calcidiol to Inactive Vitamin D Metabolites)
Ionized Calcium (in Addition to Total Calcium) Should Be Measured to More Accurately Assess Calcium Levels
The Total Serum Calcium Level Does Not Accurately Reflect the Ionized Calcium Concentration in Patients with Hypoalbuminemia/Hyperalbuminemia, Since Calcium is Bound to Albumin
In Addition, Since the Binding of Calcium to Albumin is pH-Dependent, the Amount of Free Calcium May Be Altered by an Acid-Base Disorder (Such as Metabolic Acidosis, Which May Occur in the Setting of Acute Kidney Injury) or by the Rapid Correction of an Acid-Base Disorder
Management
In the Setting of Acute Kidney Injury (AKI) with Hypocalcemia, Hyperphosphatemia Should Be Treated with Oral Phosphate Binders
Oral Phosphate Binder Treatment is Frequently Sufficient to Improve the Hypocalcemia
In the Setting of Hyperphosphatemia-Induced Hypocalcemia, the Dose of Calcium Supplementation Should Be Limited to Ameliorate Clinical Symptoms and Not Necessarily to Target a Normal Serum Calcium Level (Which Can Increase the Calcium-Phosphate Product to a Level Which Can Promote Precipitation)
Prospective Study of Hypocalcemia in Patients with Acute Pancreatitis (Ann Gastroenterol, 2016) [MEDLINE]
Approximately 35.2% of Patients Had Hypocalcemia
Mechanisms
Saponification of Calcium Soaps within the Inflamed Pancreas and Abdominal Cavity (J Bone Miner Res, 1990) [MEDLINE]
Diagnosis
Parathyroid Hormone (PTH) Levels are Typically Elevated (But May Be Variable) (Br J Surg, 1994) [MEDLINE]
Clinical
Prospective Study of Hypocalcemia in Patients with Acute Pancreatitis (Ann Gastroenterol, 2016) [MEDLINE]
Approximately 35.2% of Patients Had Hypocalcemia
Patients with Hypocalcemia Had Significantly Higher Frequency of Persistent Organ Failure, Mortality, and Need for Intervention (P<0.05)
Approximately 32.4% of the Patients with Hypocalcemia Had Tetany
Patients with Tetany Had Significantly Lower Serum Corrected Calcium and Ionized Calcium Levels, as Compared to Patients with Asymptomatic Hypocalcemia (P<0.05)
Patients with Tetany Had Significantly Higher Mortality Rates, as Compared to Patients with Asymptomatic Hypocalcemia (100% vs. 8%; P = 0.00001) as Well as Persistent Organ Failure (100% vs. 32%; P = 0.000006)
Hypocalcemia is Common in the Setting of Critical Illness or Postoperative State (Approaching 80-90% of Cases) (Ann Intern Med, 1987) [MEDLINE] (Am J Med, 1988) [MEDLINE] (Am J Kidney Dis, 2001) [MEDLINE]
Tumor Cells Have 4x as Much Phosphate as Normal Cells
When the Calcium Concentration Times the Phosphate Concentration (Calcium Phosphate Product) is >60 mg2/dL2, There is an Increased Risk of Calcium Phosphate Precipitation in the Renal Tubules (Which Can Result in Acute Kidney Injury) and the Heart (Which Can Result in Arrhythmias)
Renal Replacement Therapy (Dialysis) May be Required if the Calcium Phosphate Product is ≥70 mg2/dL2
Etiology of Chronic Hyperphosphatemia
Decreased Phosphate Clearance Due to Chronic Kidney Disease
Results in Chronic Hyperphosphatemia, Causing Hypocalcemia
In These Cases, Primary Impairment of Calcitriol Synthesis (Resulting in Decreased Intestinal Calcium Absorption) Further Exacerbates the Hypocalcemia
Mechanisms
Hyperphosphatemia Results in Calcium Deposition, Mostly in Bone (But Also in Extraskeletal Tissues)
In a Study of Advanced Prostate Cancer (n = 131), 34% of Patients Had Elevated Parathyroid Hormone (PTH) Levels and 56% Had Decreased Ionized Calcium Levels (J Clin Endocrinol Metab, 2001) [MEDLINE]
Mechanisms
Due to Deposition of Calcium in the Newly Formed Bone Around the Tumor (Am J Med, 1981) [MEDLINE] (J Clin Endocrinol Metab, 2001) [MEDLINE]
Hypocalcemia is More Frequently Seen When Potent Bisphosphonates (Such as Zoledronate) are Used and in Patients with Underlying Vitamin D Deficiency, Unrecognized Hypoparathyroidism, or Chronic Kidney Disease
Pharmacology
Bisphosphonates Reduce Osteoclastic Bone Resorption
Severe Denosumab-Induced Hypocalcemia Has Been Reported (JCEM Case Rep, 2025) [MEDLINE]
Pharmacology
Denosumab is a Fully Human Monoclonal Antibody to the Receptor Activator of Nuclear Factor Kappa B Ligand (RANKL), Which is an Osteoclast Differentiating Factor
Other Drugs/Toxins
5-Fluorouracil (5-FU) and Leucovorin (see 5-Fluorouracil)
Epidemiology
Hypocalcemia Occurs in Approximately 65% of Cases
Physiology
Probably Due to a Decrease in Calcitriol Production
Dengue Fever Has Been Associated with Hypocalcemia (Int J Crit Illn Inj Sci, 2014) [MEDLINE]
Physiology
Likely Multifactorial
Clinical
As Suggested in In Vitro Studies, Derangements of Calcium Homeostasis are Likely to Be Associated with Myocardial Dysfunction and Cardiac Arrhythmias in the Setting of Dengue Virus Infection
Hypocalcemia is a Common Manifestation of Hydrofluoric Acid Toxicity (J Trauma, 1988) [MEDLINE]
Physiology
Fluoride Ions Bind to Calcium and Magnesium [LINK]
Postoperative Hypocalcemia
Physiology
Postoperative Hypocalcemia May Occur During or Soon After Surgery in Patients Who Have Received Large Amounts of Citrate-Containing Blood Products
Postoperative Hypocalcemia May Occur Even in Cases Where No Blood Products Have Been Given (J Clin Endocrinol Metab, 1999) [MEDLINE]
Due to Volume Expansion and Hypoalbuminemia
Ionized Calcium is Normal in Most (But Not All) of These Cases
Physiology
Storage of Calcium in the Body
>99% of the Calcium in the Body is Stored as Hydroxyapatite in Bones
Calcium in the Form of Hydroxyapatite Provides Skeletal Strength as well as Serving as a Reservoir for Calcium to Be Released into the Serum
In the Cell, Calcium is Primarily Bound to Calmodulin
Mechanisms of Calcium Transport in the Blood (J Clin Invest, 1970) [MEDLINE] (Lancet, 1998) [MEDLINE]
Calcium Bound to Serum Proteins (Predominantly Albumin): 40-45%
Calcium Bound to Small Inorganic/Organic Anions (Phosphate, Citrate, Sulfate, Lactate, etc): 15%
Free (Ionized) Calcium: 40-45%
Ionized Calcium Concentration is Tightly Regulated by Parathyroid Hormone and Vitamin D
Only the Ionized Calcium is Metabolically Active (i.e. Transportable into Cells)
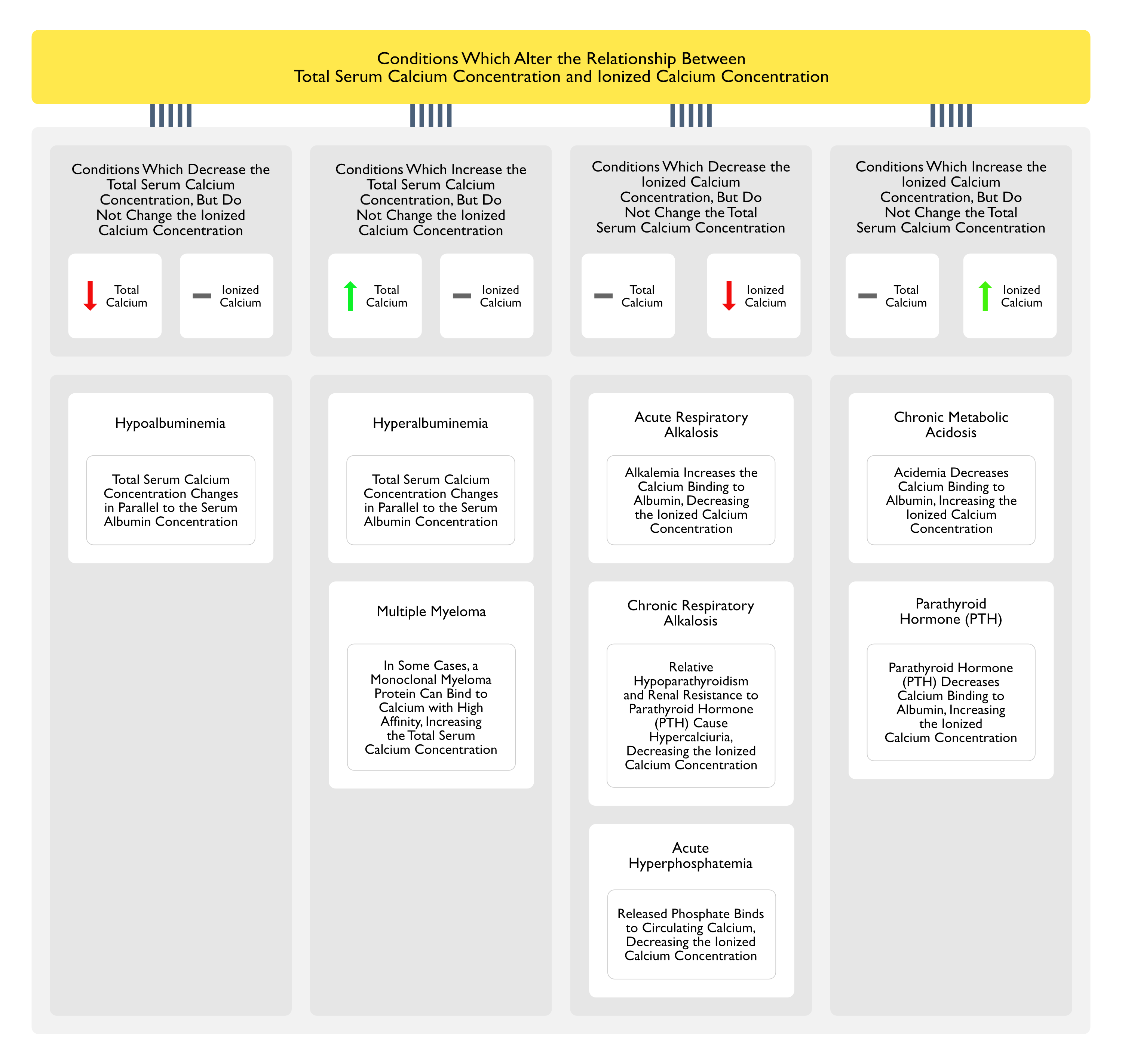
Relationship Between Total Serum Calcium Concentration and Ionized Calcium Concentration
General Comments
Normal Range of Total Serum Calcium Concentration (Varies by Laboratory): 8.5-10.5 mg/dL (2.12 to 2.62 mmol/L)
Wide Range of Normal Calcium Values is Accounted for by Individual Variations in the Serum Albumin Concentration and Hydration Status
Measurement of the Total Serum Calcium Concentration Can Be Misleading, Since There Can Be a Discordance Between Total Serum Calcium Concentration and the Ionized Calcium Concentration (J Clin Endocrinol Metab, 1978) [MEDLINE]
Normal Range of Ionized Calcium Concentration (Adult): 1.16-1.31 mmol/L (4.65-5.25 mg/dL)
When Albumin and Other Serum Protein Concentrations Vary Significantly, Total Serum Calcium Levels May Vary
However, the Ionized Calcium Concentration (Which is Hormonally Regulated by Parathyroid Hormone and Vitamin D) Remains Relatively Stable
Conditions Which Decrease the Total Serum Calcium Concentration, But Do Not Change the Ionized Calcium Concentration
Total Serum Calcium Concentration Changes in Parallel to the Serum Albumin Concentration
In the Setting of Hypoalbuminemia (Due to Liver Disease, Renal Disease, etc), Total Serum Calcium Concentration Decreases
Historical Correction of Total Serum Calcium Concentration for Serum Albumin
Total Serum Calcium Decreases by Approximately 0.8 mg/dL (0.2 mmol/L) for Every 1.0 g/dL (10 g/L) Decrease in the Serum Albumin Concentration
Despite the Widespread Use of This Equation, the Accuracy of This Correction is Believed to Be Poor, Particularly in Patients with Critical Illness and Advanced Chronic Kidney Disease (Crit Care Med, 2003) [MEDLINE] (J Am Soc Nephrol, 2008) [MEDLINE] (Clin J Am Soc Nephrol, 2010) [MEDLINE] (Semin Dial, 2010) [MEDLINE] (Scand J Clin Lab Invest, 2017) [MEDLINE] (BMJ Open, 2018) [MEDLINE] (Clin Chem, 2018) [MEDLINE]
Poor Clinical Accuracy of This Equation May Be Explained by Metabolic Acidosis, Which Leads to an Underestimate of the Ionized Calcium Concentration
Some Studies Cite the Sensitivity of This Correction Equation at Only 5% (JPEN J Parenter Enteral Nutr, 2004) [MEDLINE]
More Modern Methods to Correct the Total Serum Calcium Concentration for Serum Albumin Have Not Been Widely Validated (and are Therefore, are Not Widely Used) (JPEN J Parenter Enteral Nutr, 2004) [MEDLINE] (Clin J Am Soc Nephrol, 2018) [MEDLINE] (J Appl Lab Med, 2020) [MEDLINE] (Clin Chim Acta, 2022) [MEDLINE]
Consequently, the Measurement of Ionized Calcium Remains the Gold Standard to Assess Calcium Status
If the Total Serum Calcium Concentration is Decreased, But the Ionized Calcium Concentration is Normal, This is Termed “Pseudohypocalcemia”
Conditions Which Increase the Total Serum Calcium Concentration, But Do Not Change the Ionized Calcium Concentration
Total Serum Calcium Concentration Changes in Parallel to the Serum Albumin Concentration
In the Setting of Hyperalbuminemia (Due to Extracellular Volume Deplteion, Fluid Movement Out of the Vascular Space, High Protein Diet, etc), Total Serum Calcium Concentration Increases
If the Total Serum Calcium Concentration is Increased, But the Ionized Calcium Concentration is Normal, This is Termed “Pseudohypercalcemia”
In Some Cases, a Monoclonal Myeloma Protein Can Bind to Calcium with High Affinity, Increasing the Total Serum Calcium Concentration
Since Multiple Myeloma Can Cause True Hypercalcemia Due to Osteolytic Bone Metastases, Measuring an Ionized Calcium is Nescssary to Aid in the Diagnosis This Entity
Hyperproteinemia Can Also Cause a Spurious Increase in Serum Phsophate Concentration (see Hyperphosphatemia) (BMJ, 1989) [MEDLINE]
Due to Interference with the Molybdate Assay Used to Measure the Serum Phosphate Concentration
Conditions Which Decrease the Ionized Calcium Concentration, But Do Not Change the Total Serum Calcium Concentration
Alkalemia Increases the Calcium Binding to Albumin, Decreasing the Ionized Calcium Concentration (Eur J Clin Invest, 1982) [MEDLINE]
Decrease in Ionized Calcium Concentration is Approximately 0.16 mg/dL (0.04 mmol/L or 0.08 mEq/L) for Each 0.1 Unit Increase in the pH
Clinical
For This Reason, Hyperventilation with Acute Respiratory Alkalosis Can Result in Clinical Symptoms of Hypocalcemia (Such as Muscle Cramps, Paresthesias, Tetany, and Seizures)
Similarly, In Vitro Changes in the pH in Whole Blood or Serum Laboratory Specimens Can Result in Changes in the Ionized Calcium Concentration (Lab Med, 2002) [MEDLINE]
In the Setting of Chronic Kidney Disease (CKD) with Coexisting Underlying Hypocalcemia, Bicarbonate Therapy (or Dialysis) Can Increase the Serum pH, Resulting in a Decreased Ionized Calcium Concentration and Clinical Symptoms of Hypocalcemia (Am J Kidney Dis, 1997) [MEDLINE] (Nephron, 2001) [MEDLINE]
Although the Mechanism is Unclear, It Appears to Be Due to Relative Hypoparathyroidism and Renal Resistance to Parathyroid Hormone (PTH) with Resultant Hypercalciuria, Decreasing the Ionized Calcium Concentration (Kidney Int, 1992) [MEDLINE]
Due to Cellular Breakdown with Phosphate Release, the Released Phosphate Binds to Circulating Calcium, Decreasing the Ionized Calcium Concentration
In Addition, in a Short Period of Time, Calcium-Phosphate Precipitates and Deposits in Soft Tissues, Additionally Resulting in a Decreased Total Serum Calcium Concentration
Conditions Which Increase the Ionized Calcium Concentration, But Do Not Change the Total Serum Calcium Concentration
Acidemia Decreases Calcium Binding to Albumin, Increasing the Ionized Calcium Concentration
Parathyroid Hormone (PTH)
Mechanism
Parathyroid Hormone Decreases Calcium Binding to Albumin, Increasing the Ionized Calcium Concentration (J Clin Endocrinol Metab, 1979) [MEDLINE]
However, Since Sensitivities of Total Serum Calcium Concentration and Ionized Calcium Concentration were the Same in the Diagnosis of Primary Hyperparathyrodism, the Effect of PTH on Protein Binding of Calcium May Not Have Clinical Significance (Clin Biochem, 2011) [MEDLINE]
Major Factors Which Affect Serum Calcium Concentration
Parathyroid Hormone (PTH)
Parathyroid Hormone (PTH) is Secreted Almost Immediately in Response to a Small Decrease in the Ionized Calcium Concentration (Which is Sensed by the Calcium-Sensing Receptor/CaSR in the Parathyroid Gland)
Parathyroid Hormone (PTH) Increases Calcium Absorption in the Distal Tubule, Consequently Decreasing Renal Calcium Excretion
Parathyroid Hormone (PTH) Increases Bone Resorption of Calcium
Parathyroid Hormone (PTH) Increases Renal Production of 1,25-Dihydroxyvitamin D, Which Functions to Increase Intestinal Calcium Absorption
Vitamin D
Vitamin D is Enzymatically Converted in the Liver to 25-Hydroxyvitamin D (the Major Circulating Form of Vitamin D) and Then in the Kidney to 1,25-Dihydroxyvitamin D3 (Calcitriol; the Active Form of Vitamin D)
The Most Important Biological Function of Vitamin D is to Promote Enterocyte Differentiation and the Intestinal Absorption of Calcium
Lesser Stimulation of Intestinal Phosphate Absorption
Direct Suppression of Parathyroid Hormone (PTH) Release from the Parathyroid Gland
Regulation of Osteoblast Function
Permissively Allowing Parathyroid Hormone (PTH)-Induced Osteoclast Activation and Bone Resorption
Normal Range (Varies by Laboratory): 8.5-10.5 mg/dL (2.12 to 2.62 mmol/L)
Level Below the Lower End of this Normal Range is Considered Hypocalcemia
Wide Range of Normal Calcium Values is Accounted for by Individual Variations in the Serum Albumin Concentration and Hydration Status
Measurement of the Total Serum Calcium Concentration Can Be Misleading, Since There Can Be a Discordance Between Total Serum Calcium Concentration and Ionized Calcium Concentration (J Clin Endocrinol Metab, 1978) [MEDLINE]
Ionized Calcium
Normal Range of Ionized Calcium
Normal Range: 1.16 to 1.31 mmol/L (4.65 to 5.25 mg/dL)
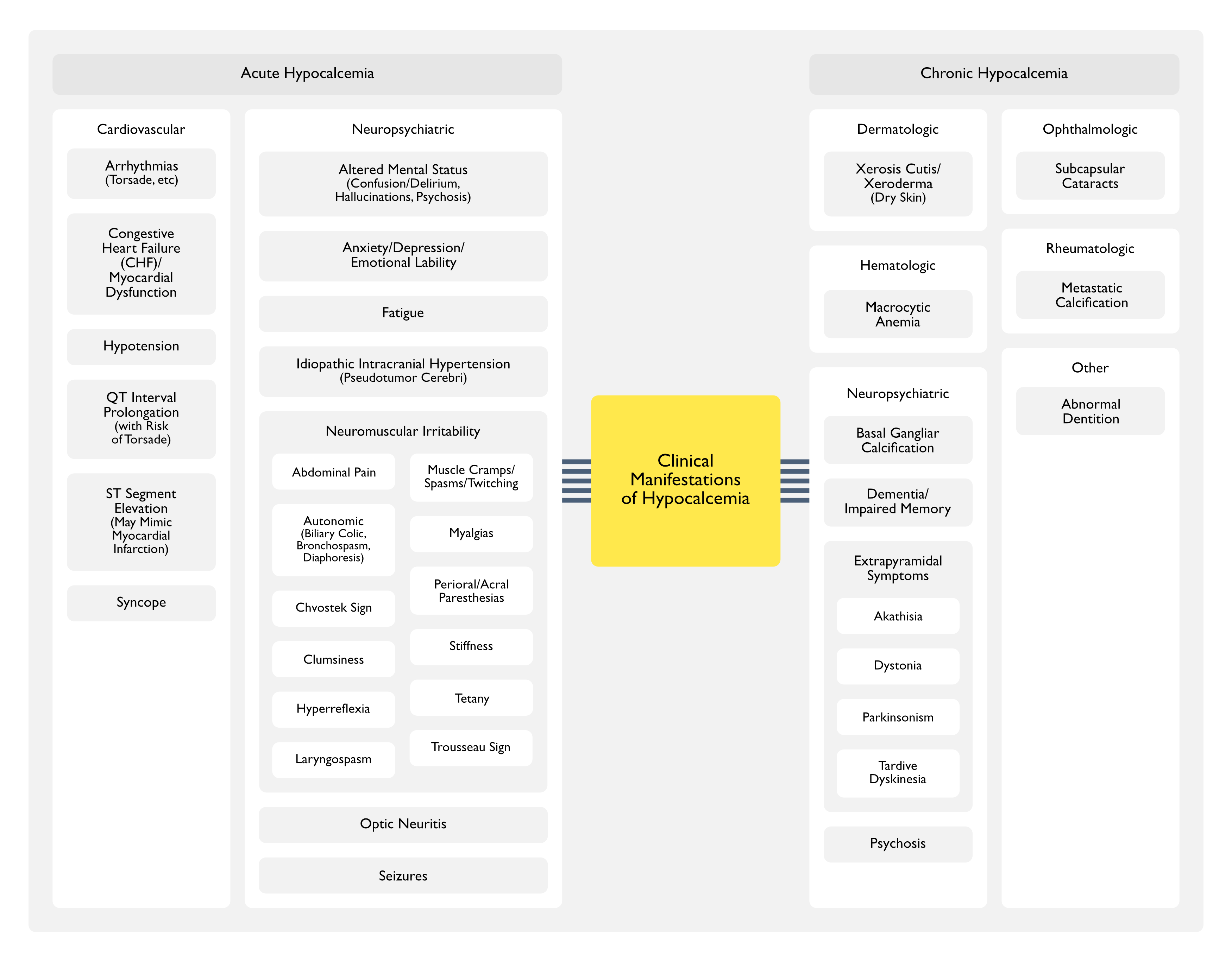
Clinical Manifestations
Acute Hypocalcemia
Cardiovascular Manifestations
Arrhythmias
Physiology
Hypocalcemia (Frequently Seen in the Setting of Chronic Kidney Disease) Results in ST Segment Prolongation and QT Interval Prolongation (J Emerg Med, 2004) [MEDLINE] (Cardiol J, 2011) [MEDLINE]
Clinical
Torsades de Pointes (Polymorphic Ventricular Tachycardia Associated with a QT Prolongation) Can Be Triggered by Hypocalcemia, But Occurs Far Less Frequently than it Does in the Setting of Hypokalemia or Hypomagnesemia
Although Electrocardiographic Conduction Abnormalities are Common, Serious Hypocalcemia-Induced Arrhythmias (Heart Block, Ventricular Arrhythmias, etc), are Uncommon
Cases of Hypocalcemia-Associated Hypotension Have Been Extensively Reported (Am J Kidney Dis, 1994) [MEDLINE] (Am J Kidney Dis, 2015) [MEDLINE] (Hemodial Int, 2016) [MEDLINE]
Hypocalcemia-Associated Hypotension is Most Commonly Seen When it is Rapidly Induced by Ethylenediaminetetraacetic Acid (EDTA), Transfusion of Citrated Blood Products, or with the Use of Low Calcium Dialysate in Patients Undergoing Dialysis (Anesth Analg, 1976) [MEDLINE] (Am J Kidney Dis, 1994) [MEDLINE] (Am J Kidney Dis, 2015) [MEDLINE] (Hemodial Int, 2016) [MEDLINE]
Hypocalcemia-Induced Hypotension May Be Observed During Continuous Renal Replacement Therapy (CRRT) (J Crit Care, 2021) [MEDLINE]
Physiology
Calcium is Required for Vascular Smooth Muscle Contractility (Microcirculation, 2013) [MEDLINE]
QT Interval Prolongation with Increased Risk of Torsade (see Torsade)
Physiology
Hypocalcemia (Frequently Seen in the Setting of Chronic Kidney Disease) Results in ST Segment Prolongation and QT Interval Prolongation (J Emerg Med, 2004) [MEDLINE] (Eur J Cardiovasc Prev Rehabil, 2005) [MEDLINE] (J Electrocardiol, 2007) [MEDLINE] (Cardiol J, 2011) [MEDLINE]
Hypocalcemia Prolongs Phase 2 of the Action Potential (with the Impact Modulated by the Rate of CHange of Serum Calcium Concentration and Function of the Myocyte Calcium Channels)
QT Prolongation is Associated with Early After-Depolarizations and Triggered Arrhythmias
Clinical
Torsades de Pointes (Polymorphic Ventricular Tachycardia Associated with a QT Prolongation) Can Be Triggered by Hypocalcemia, But Occurs Far Less Frequently than it Does in the Setting of Hypokalemia or Hypomagnesemia
Although Electrocardiographic Conduction Abnormalities are Common, Serious Hypocalcemia-Induced Arrhythmias (Heart Block, Ventricular Arrhythmias, etc), are Uncommon
ST-Segment Elevation (Mimicking ST Elevation Myocardial Infarction)
Epidemiology
Cases Have Been Reported (Cardiol J, 2022) [MEDLINE]
Tetany is Most Commonly Observed in the Setting of Acute Hypercalcemia
Patients with a Gradual Decline in Serum Calcium Tend to Have Fewer Symptoms at the Same Calcium Level than Patients with Acute Hypocalcemia (Endocrinol Metab Clin North Am, 1993) [MEDLINE]
Tetany Usually Only Occurs when Ionized Calcium Falls to Below 1.10 mmol/L (Corresponding to a Total Serum Calcium of Approximately 7-7.5 mg/dL)
Other Name for Sign: “main d’accoucheur” (French for “hand of the obstetrician”) because it resembles the position of an obstetrician’s hand in delivering a baby
Inflated Blood Pressure Cuff for 3 min Elicits Carpopedal Spasm in the Hand/Forearm
In Hypocalcemia-Associated Seizures, the Electroencephalogram (EEG) Demonstrates Both Spikes (“Convulsive Effect”) and Bursts of High-Voltage, Paroxysmal Slow Waves (Arch Neurol, 1972) [MEDLINE]
Clinical
General Comments
Seizures May Be the Sole Presenting Symptom (Clin EEG Neurosci, 2004) [MEDLINE] (Epileptic Disord, 2004) [MEDLINE] (ASN Neuro, 2015) [MEDLINE]
Systematic Review of Parenteral Calcium Replacement in Critical Care Patients (Cochrane Database Syst Rev, 2008) [MEDLINE]: no evidence that parenteral calcium replacement improves outcome in critically ill patients
Agents
Calcium Chloride (in 10 ml = 10%) (see Calcium Chloride): 1 amp over 30-60 min
The incidence of parathyroid and other antibodies in the sera of patients with idiopathic hypoparathyroidism. Clin Exp Immunol. 1966;1(2):119 [MEDLINE]
Massive blood replacement: correlation of ionized calcium, citrate, and hydrogen ion concentration. Anesth Analg 1979; 58:274-278 [MEDLINE]
Two types of autoimmune Addison’s disease associated with different polyglandular autoimmune (PGA) syndromes. Medicine (Baltimore). 1981;60(5):355 [MEDLINE]
Hypocalcemia with osteoblastic metastases in patient with prostate carcinoma. A cause of secondary hyperparathyroidism. Am J Med. 1981;71(1):184 [MEDLINE]
Hypoparathyroidism in Wilson’s disease. N Engl J Med. 1983;309(15):873 [MEDLINE]
The influence of hypermagnesemia on serum calcium and parathyroid hormone levels in human subjects. N Engl J Med. 1984;310(19):1221 [MEDLINE]
The multifactorial basis for hypocalcemia during sepsis. Studies of the parathyroid hormone-vitamin D axis. Ann Intern Med. 1987;107(1):36 [MEDLINE]
Intraperitoneal free fatty acids induce severe hypocalcemia in rats: a model for the hypocalcemia of pancreatitis. J Bone Miner Res. 1990;5(12):1249 [MEDLINE]
Symptomatic hypocalcaemia associated with metastatic invasion of the parathyroid glands. Br J Hosp Med. 1990;43(1):72 [MEDLINE]
Hypocalcemia induced during major and minor abdominal surgery in humans. J Clin Endocrinol Metab. 1999;84(8):2654 [MEDLINE]
Ionized hypocalcemia during sepsis. Crit Care Med 2000; 28:266-268 [MEDLINE]
Hypocalcemic and normocalcemic hyperparathyroidism in patients with advanced prostatic cancer. J Clin Endocrinol Metab. 2001;86(9):4133 [MEDLINE]
Hypocalcemia: a pervasive metabolic abnormality in the critically ill. Am J Kidney Dis. 2001;37(4):689. [MEDLINE]
Electrolyte disturbances in the intensive care unit. Semin Dial 2006; 19:496-501 [MEDLINE]
Hypoparathyroidism in transfusion-dependent patients with beta-thalassemia. J Bone Miner Metab. 2006;24(2):138 [MEDLINE]
Endocrine complications in patients with Thalassaemia Major. Pediatr Endocrinol Rev. 2007;5(2):642 [MEDLINE]
Calcium homeostasis during magnesium treatment in aneurysmal subarachnoid hemorrhage. Neurocrit Care 2008;8(3):413 [MEDLINE]
Dengue and calcium. Int J Crit Illn Inj Sci. 2014 Oct-Dec;4(4):314-6. doi: 10.4103/2229-5151.147538 [MEDLINE]
Hyperphosphatemia is associated with high mortality in severe burns. PLoS One. 2018; 13(1): e0190978. Published online 2018 Jan 9. doi: 10.1371/journal.pone.0190978 [MEDLINE]
Metastases to the Parathyroid Glands: A Comprehensive Literature Review of 127 Reported Cases. Head Neck Pathol. 2018 Dec; 12(4): 534–541. Published online 2017 Sep 5. doi: 10.1007/s12105-017-0850-x [MEDLINE]
Transfusion-Related Hypocalcemia After Trauma. World J Surg. 2020 Nov;44(11):3743-3750. doi: 10.1007/s00268-020-05712-x [MEDLINE]
Severe hypocalcemia due to hypoparathyroidism associated with HIV: A case report. Bone Rep. 2021 Aug 20:15:101119. doi: 10.1016/j.bonr.2021.101119. eCollection 2021 Dec [MEDLINE]
Endocrine-related adverse conditions induced by tyrosine kinase inhibitors. Ann Endocrinol (Paris). 2023 May;84(3):374-381. doi: 10.1016/j.ando.2023.03.009 [MEDLINE]
Refractory Denosumab-induced Hypocalcemia in a High-risk Patient With Osteoblastic Metastatic Prostate Adenocarcinoma. JCEM Case Rep. 2025 Jun 13;3(8):luaf121. doi: 10.1210/jcemcr/luaf121. eCollection 2025 Aug [MEDLINE]
Physiology
Ionized calcium in normal serum, ultrafiltrates, and whole blood determined by ion-exchange electrodes. J Clin Invest. 1970;49(2):318 [MEDLINE]
Failure of total calcium corrected for protein, albumin, and pH to correctly assess free calcium status. J Clin Endocrinol Metab. 1978;46(6):986 [MEDLINE]
Relationship of free and total calcium in hypercalcemic conditions. J Clin Endocrinol Metab. 1979;48(3):393 [MEDLINE]
The effect of respiratory and metabolic acid-base changes on ionized calcium concentration: in vivo and in vitro experiments in man and rat. Eur J Clin Invest. 1982;12(6):451 [MEDLINE]
Pseudohyperphosphataemia in multiple myeloma. BMJ. 1989;299(6712):1381 [MEDLINE]
Chronic respiratory alkalosis induces renal PTH-resistance, hyperphosphatemia and hypocalcemia in humans. Kidney Int. 1992;42(3):727 [MEDLINE]
Hypocalcemic tetany and metabolic alkalosis in a dialysis patient: an unusual event. Am J Kidney Dis. 1997;30(3):440 [MEDLINE]
Direct effect of the correction of acidosis on plasma parathyroid hormone concentrations, calcium and phosphate in hemodialysis patients: a prospective study. Nephron. 2001;87(3):257 [MEDLINE]
pH effects on measurements of ionized calcium and ionized magnesium in blood. Arch Pathol Lab Med. 2002;126(8):947 [MEDLINE]
Albumin-adjusted calcium is not suitable for diagnosis of hyper- and hypocalcemia in the critically ill. Crit Care Med. 2003;31(5):1389 [MEDLINE]
Accuracy of methods to estimate ionized and “corrected” serum calcium concentrations in critically ill multiple trauma patients receiving specialized nutrition support. JPEN J Parenter Enteral Nutr. 2004;28(3):133 [MEDLINE]
Pitfalls of measuring total blood calcium in patients with CKD. J Am Soc Nephrol. 2008;19(8):1592 [MEDLINE]
Measuring total blood calcium displays a low sensitivity for the diagnosis of hypercalcemia in incident renal transplant recipients. Clin J Am Soc Nephrol. 2010;5(11):2085 [MEDLINE]
Physiology and pathophysiology of the calcium-sensing receptor in the kidney. Am J Physiol Renal Physiol. 2010;298(3):F485 [MEDLINE]
Is the calcium correct? Measuring serum calcium in dialysis patients. Semin Dial. 2010 May;23(3):283-9 [MEDLINE]
Physiology and pathophysiology of the calcium-sensing receptor in the kidney. Am J Physiol Renal Physiol. 2010;298(3):F485 [MEDLINE]
Biochemical diagnosis of primary hyperparathyroidism: Analysis of the sensitivity of total and ionized calcium in combination with PTH. Clin Biochem. 2011;44(10-11):849 [MEDLINE]
Albumin adjustment of total calcium does not improve the estimation of calcium status. Scand J Clin Lab Invest. 2017;77(6):442 [MEDLINE]
Should total calcium be adjusted for albumin? A retrospective observational study of laboratory data from central Norway. BMJ Open. 2018;8(4):e017703 [MEDLINE]
Misclassification of Calcium Status Based on Albumin-Adjusted Calcium: Studies in a Tertiary Hospital Setting. Clin Chem. 2018;64(12):1713 [MEDLINE]
Anion Gap as a Determinant of Ionized Fraction of Divalent Cations in Hemodialysis Patients. Clin J Am Soc Nephrol. 2018;13(2):274 [MEDLINE]
Predicting Ionized Hypocalcemia in Critical Care: An Improved Method Based on the Anion Gap. J Appl Lab Med. 2020;5(1):4 [MEDLINE]
Novel methods of predicting ionized calcium status from routine data in critical care: External validation in MIMIC-III. Clin Chim Acta. 2022;531:375 [MEDLINE]
Clinical Manifestations
Cardiovascular
Hypocalcemic hypotension. JAMA. 1973 Oct 15;226(3):355-6. doi: 10.1001/jama.1973.03230030067031 [MEDLINE]
Cardiac failure associated with hypocalcemia. Anesth Analg. 1976;55(1):34 [MEDLINE]
Hypocalcemic heart failure. Am J Med. 1985;78(6 Pt 1):1033 [MEDLINE]
Improvement of hypocalcemic cardiomyopathy by correction of serum calcium level. Am Heart J. 1985;109(3 Pt 1):611 [MEDLINE]
Hypocalcemic myocardial dysfunction: short- and long-term improvement with calcium replacement. Am Heart J. 1990;120(2):381 [MEDLINE]
Hypocalcemic heart failure in end-stage renal disease. Am J Nephrol 1990;10(2):167-70. doi: 10.1159/000168073 [MEDLINE]
Hypocalcemic myocardial dysfunction: short- and long-term improvement with calcium replacement. Am Heart J. 1990;120(2):381 [MEDLINE]
Exacerbation of latent heart failure by mild hypocalcemia after parathyroidectomy in a long-term hemodialysis patient. Nephron. 1992;60(4):482 [MEDLINE]
Hypocalcemic cardiomyopathy in a patient with idiopathic hypoparathyroidism. Intern Med. 1992;31(4):561 [MEDLINE]
Refractory hypotension associated with hypocalcemia and renal disease. Am J Kidney Dis. 1994;23(3):430 [MEDLINE]
Congestive heart failure caused by vitamin D deficiency? Acta Paediatr. 1995;84(1):106 [MEDLINE]
Corrected QT interval (QTc) prolongation and syncope associated with pseudohypoparathyroidism and hypocalcemia. J Pediatr. 2000 Mar;136(3):404-7. doi: 10.1067/mpd.2000.103447 [MEDLINE]
Risk factors for prolonged QTc among US adults: Third National Health and Nutrition Examination Survey. Eur J Cardiovasc Prev Rehabil. 2005;12(4):363 [MEDLINE]
Thymoma-associated hypocalcemic crisis. South Med J. 2005 Aug;98(8):836-8. doi: 10.1097/01.SMJ.0000163313.35350.79 [MEDLINE]
Reversible hypocalcemic heart failure with T wave alternans and increased QTc dispersion in a patient with chronic renal failure after parathyroidectomy. Clin Nephrol 2006 Jan;65(1):65-70. doi: 10.5414/cnp65065 [MEDLINE]
Hereditary long QT syndrome due to autoimmune hypoparathyroidism in autoimmune polyendocrinopathy-candidiasis-ectodermal dystrophy syndrome. J Electrocardiol. 2007;40(6):504 [MEDLINE]
Reversible congestive heart failure related to profound hypocalcemia secondary to hypoparathyroidism. Am J Med Sci 2007 Apr;333(4):226-9. doi: 10.1097/MAJ.0b013e318039b9c6 [MEDLINE]
Electrolyte disorders and arrhythmogenesis. Cardiol J. 2011;18(3):233-45 [MEDLINE]
Facility Dialysate Calcium Practices and Clinical Outcomes Among Patients Receiving Hemodialysis: A Retrospective Observational Study. Am J Kidney Dis. 2015 Oct;66(4):655-65 [MEDLINE]
Dialysate-induced hypocalcemia presenting as acute intradialytic hypotension: A case report, safety review, and recommendations. Hemodial Int. 2016;20(2):E8 [MEDLINE]
Hypocalcemia is associated with hypotension during CRRT: A secondary analysis of the Acute Renal Failure Trial Network Study. J Crit Care. 2021 Oct:65:261-267. doi: 10.1016/j.jcrc.2021.07.008 [MEDLINE]
Severe hypocalcemia mimicking acute ST-segment elevation myocardial infarction: Paradigmatic case and review of literature. Cardiol J. 2022;29(4):710-713. doi: 10.5603/CJ.a2022.0048 [MEDLINE]
Hypocalcaemia in an adult: the importance of not overlooking the cause. BMJ Case Rep. 2018 Apr 5;2018. pii: bcr-2017-224108. doi: 10.1136/bcr-2017-224108 [MEDLINE]
Clinical Presentation of Hypoparathyroidism. Front Horm Res. 2019;51:139-146. doi: 10.1159/000491044 [MEDLINE]
Neurologic
Optic neuritis in hypoparathyroidism. Neurology. 1976;26(5):451 [MEDLINE]
Cataracts and pseudotumor cerebri in an infant with vitamin D-deficiency rickets. J Pediatr. 1977;90(2):252 [MEDLINE]
Hypoparathyroidism and pseudotumor cerebri: an infrequent clinical association. Can J Neurol Sci. 1987;14(4):622 [MEDLINE]
Bisphosphonate-induced Severe Hypocalcemia – A Case Report. J Bone Metab. 2012 Nov;19(2):139-45. doi: 10.11005/jbm.2012.19.2.139 [MEDLINE]
Hypocalcemia-induced seizure: demystifying the calcium paradox. ASN Neuro. 2015 Mar 24;7(2):1759091415578050. doi: 10.1177/1759091415578050 [MEDLINE]
Hypocalcemic tetany: a simple bedside marker of poor outcome in acute pancreatitis. Ann Gastroenterol. 2016 Apr-Jun;29(2):214-20. doi: 10.20524/aog.2016.0015 [MEDLINE]
Seizures
Electroencephalographic criteria of hypocalcemia and hypercalcemia. Arch Neurol. 1972;26(3):218 [MEDLINE]
Anticonvulsive action of increased calcium concentration in cerebrospinal fluid. Arch Neurol. 1973;29(4):245 [MEDLINE]
Tonic-clonic seizures in a patient with primary hypoparathyroidism: a case report. Clin EEG Neurosci. 2004;35(2):97 [MEDLINE]
Hypocalcemic generalised seizures as a manifestation of iatrogenic hypoparathyroidism months to years after thyroid surgery. Epileptic Disord. 2004;6(2):85 [MEDLINE]
Other
Paraesthesiae and tetany induced by voluntary hyperventilation. Increased excitability of human cutaneous and motor axons. Brain. 1991;114 ( Pt 1B):527 [MEDLINE]
Hypocalcemic emergencies. Endocrinol Metab Clin North Am. 1993;22(2):363 [MEDLINE]
Facility Dialysate Calcium Practices and Clinical Outcomes Among Patients Receiving Hemodialysis: A Retrospective Observational Study. Am J Kidney Dis. 2015 Oct;66(4):655-65 [MEDLINE]
Treatment
Choice of calcium salt. A comparison of the effects of calcium chloride and gluconate on plasma ionized calcium. Anaesthesia. 1984 Nov;39(11):1079-82 [MEDLINE]
Calcium chloride versus calcium gluconate: comparison of ionization and cardiovascular effects in children and dogs. Anesthesiology. 1987 Apr;66(4):465-70 [MEDLINE]
Ionization and hemodynamic effects of calcium chloride and calcium gluconate in the absence of hepatic function. Anesthesiology. 1990 Jul;73(1):62-5 [MEDLINE]
Parenteral calcium for intensive care unit patients. Cochrane Database Syst Rev 2008 Oct 8; (4):CD006163. DOI: 1002/14651858.CD006163.pub2 [MEDLINE]