DSM IV-TR Definition: as an acute confusional state characterized by fluctuating mental status, inattention, and either altered level of consciousness or disorganized thinking
NIH Definition: sudden severe confusion and rapid changes in brain function that occur with physical or mental illness
Epidemiology of Intensive Care Unit (ICU)-Associated Delirium
Prevalence
General Comments
Prevalence of Delirium in Mechanically Ventilated Patients: 60-80%
Prevalence of Delirium in Non-Mechanically Ventilated Patients: 40-60%
Clinical Data
BRAIN-ICU Study of Patients with Respiratory Failure or Shock in the Medical/Surgical ICU (NEJM, 2013) [MEDLINE]: n = 821)
Delirium Developed in 74% of Cases During Hospital Stay
Outcomes At 3 Months
40% of Patients Had Impaired Global Cognition Scores that Were 1.5 SD Below the Population Mean, Similar to Scores for Patients with Moderate Traumatic Brain Injury
26% of Patients Had Scores 2 SD Below the Population Mean (similar to scores for patients with Mild Alzheimer’s Disease
Outcomes At 12 Months
Similar Persistent Cognitive Dysfunction Occurs as in Those with Moderate Traumatic Brain Injury
Similar Persistent Cognitive Dysfunction Occurs as in Those with Mild Alzheimer’s Disease
Impact of Duration of Delirium
Longer Duration of Delirium was Significantly Associated with Worse Global Cognition at 3 and 12 Months and Worse Executive Function at 3 and 12 Months
Impact of Sedative Use
Use of Sedatives or Analgesics was Not Associated with Cognitive Impairment at 3 and 12 Months
Cognitive Dysfunction was Also Independent of Age, Pre-Existing Cognitive Impairment, Presence or Severity of Coexisting Conditions, and Organ Failure During ICU Care
Systematic Review of Delirium and Outcomes in Critically Ill Patients (BMJ, 2015) [MEDLINE]
Delirium was Identified in 5,280 of 16,595 (31.8%) Critically Ill Patients Reported in 42 Studies
When compared with control patients without delirium, patients with delirium had significantly higher mortality during admission (risk ratio 2.19, 94% confidence interval 1.78 to 2.70; P<0.001) as well as longer durations of mechanical ventilation and lengths of stay in the intensive care unit and in hospital (standard mean differences 1.79 (95% confidence interval 0.31 to 3.27; P<0.001), 1.38 (0.99 to 1.77; P<0.001), and 0.97 (0.61 to 1.33; P<0.001), respectively)
Available studies indicated an association between delirium and cognitive impairment after discharge
Risk Factors for Intensive Care Unit-Associated Delirium (Synopsis of the National Institute for Health and Clinical Excellence Guideline for Prevention of Delirium; Ann Intern Med, 2011) [MEDLINE]
Studies are Conflicting as to the Association of Delirium with Systemic Corticosteroids
Study of Delirium Risk Factors in Patients with Acute Lung Injury (Crit Care Med, 2014) [MEDLINE]: systemic corticosteroids were associated with an increased risk of delirium
Prospective Cohort Study of Risk Factors for Delirium in the ICU (Int Care Med Exp, 2015) [MEDLINE]: systemic corticosteroids were not associated with an increased risk of delirium
Use of Physical Restraints During the ICU Stay May Increase the Risk of PTSD (Am J Crit Care, 2001) [MEDLINE]
Study of the Influence of Physical Restraints on Unplanned Extubation in Adult ICU Patients (Am J Crit Care, 2008) [MEDLINE]: an impaired level of consciousness on admission to the ICU and the presence of nosocomial infection increased the risk for unplanned extubation, even when physical restraints were used
Use of Physical Restraints is Associated with Sedative Use, Analgesic Use, Anti-Psychotic Drug Use, Agitation, Heavy Sedation, and Occurrence of an Adverse Event (Crit Care, 2014) [MEDLINE]: treatment characteristics predominantly predicted restraint use, as opposed to patient or hospital/ICU characteristics
Risk Factors for Intensive Care Unit-Associated Delirium (Clinical Practice Guidelines for the Management of Pain, Agitation, and Delirium in Adult Patients in the Intensive Care Unit; Critical Care Med, 2013) [MEDLINE]
Four Predominant Risk Factors for Intensive Care Unit-Associated Delirium (Grade B Evidence)
Coma is an Independent Risk factor for the Development of Intensive Care Unit-Associated Delirium (Grade B Evidence)
Medication Administration
In Mechanically Ventilated Patients, Dexmedetomidine is Associated with a Decreased Risk of Delirium, as Compared to Benzodiazepine Administration (Grade B Evidence)
Benzodiazepine Administration May Be Associated with an Increased Risk Factor for the Delirium in ICU Patients (Grade C Evidence)
Data are Unclear as the Association Between Opiate Administration and Risk of Delirium in ICU Patients (Grade B Evidence)
Data are Unclear as the Association Between Propofol Administration and Risk of Delirium in ICU Patients (Grade C Evidence)
Risk Factors for Delirium After Cardiac Surgery Requiring Cardiopulmonary Bypass (Crit Care, 2015) [MEDLINE]
Study of Statin Use and CRP in Relation to ICU Delirium (Am J Respir Crit Care Med, 2014) [MEDLINE]: prospective cohort analysis (n = 470)
In Patients Previously on Statins Prior to ICU Admission, Statin Use the Night Prior was Associated with Decreased C-Reactive Protein (CRP) and Decreased Risk of ICU Delirium the Next Day
Since Muscarinic Input Contributes to Both Pupillary Constriction and Effective Accommodation, Anticholinergic Effects Result in Mydriasis and Ineffective Accommodation (with Blurry Vision)(
“Dry as a Bone”
Since Sweat Glands are Innervated by Muscarinic Receptors, Anticholinergic Effects Result in Anhidrosis (Lack of Sweating)
“Hot as a Hare”
Since Sweat Glands are Innervated by Muscarinic Receptors, Anticholinergic Effects Result in Anhidrosis (Lack of Sweating), Culminating in Hyperthermia
“Red as a Beet”
To Compensate for the Loss of Sweat Production (as a Cooling Mechanism), Dermal Vasodilation Occurs to Dissipate Heat by Shunting Blood to the Skin
“Mad as a Hatter”
Blockade of Central Nervous System Muscarinic Receptors Results in Various Neuropsychiatric Manifestations (Agitation, Anxiety, Bizarre Behavior, Delirium, Paranoid Psychosis, Visual Hallucinations, Coma, and Seizures)
Central Nervous System Findings are Consistent with “Severe” Anticholinergic Toxicity
“Full as a Flask”
Since the Detrusor Muscle of the Bladder and the Urethral Sphincter are Both Under Muscarinic Control, Anticholinergic Effects Decrease Detrusor Contraction (Decreasing Desire to Urinate) and Prevent Normal Opening of the Urethral Sphincter (Causing Urinary Retention)
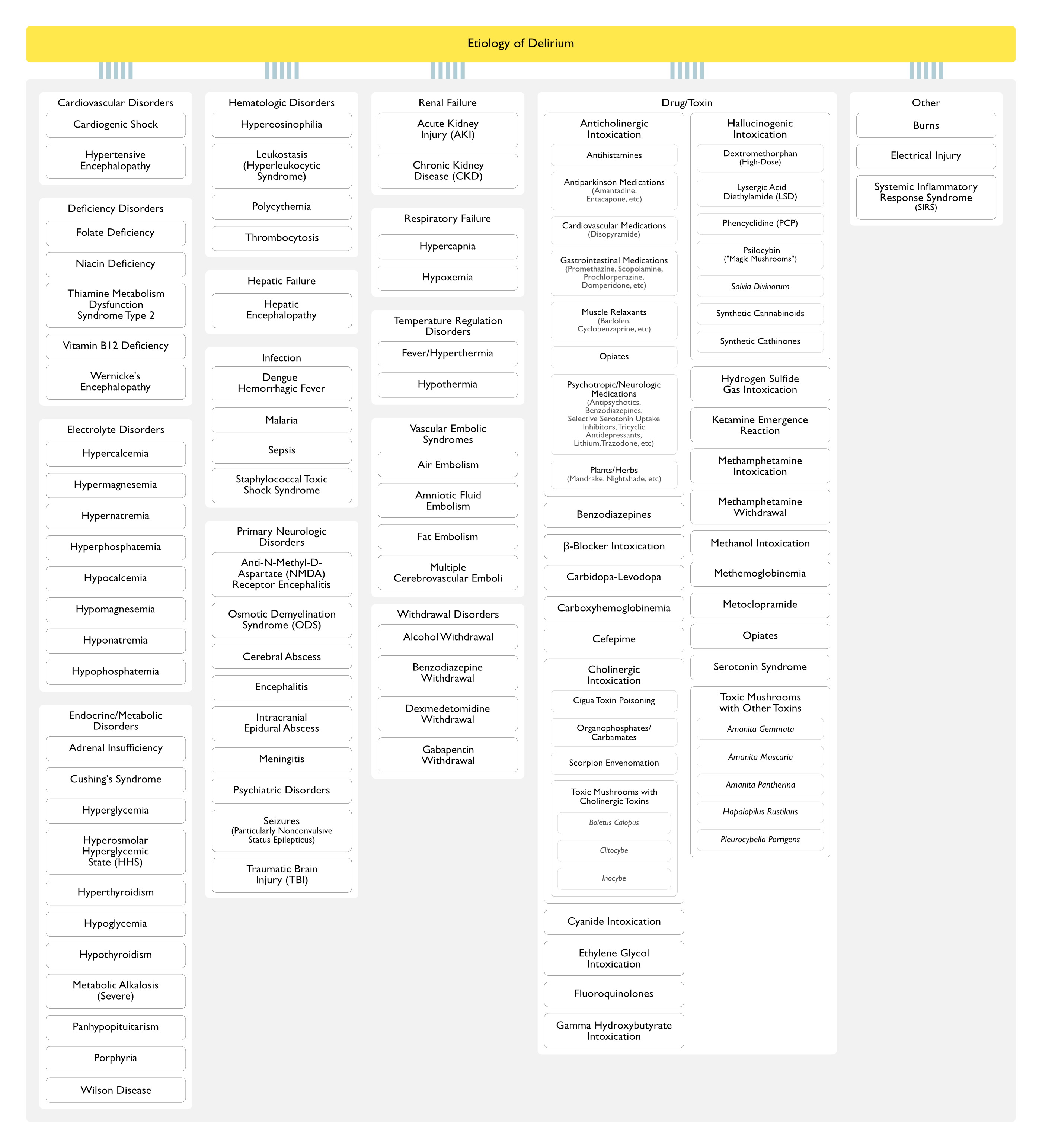
Delirium is Particularly Associated with the Use of Fluoroquinolones in Older Patients with Advanced Chronic Kidney Disease (JAMA Netw Open, 2022) [MEDLINE]
Salvia Divinorum (Diviner’s Sage, Ska María Pastora, Seer’s Sage, Yerba de la Pastora, Magic Min) (see Salvia)
Physiology
Salvia Divinorum Contains the Active Compound, Salvinorin A
By Mass, Salvinorin A is the Most Potent Naturally Occurring Hallucinogen (Active at Doses as Low as 200 µg)
Salvinorin A is a Diterpene Hallucinogen Which Functions as a Potent and Selective κ-Opioid (Kappa-Opioid) Receptor Agonist and D2 Receptor Partial Agonist
Potential Mechanisms Contributing to the Development of Delirium in the Intensive Care Unit (Handb Clin Neurol, 2017) [MEDLINE]
Aberrant Stress Response
Altered Cerebral Blood Flow
Cerebral Hypoperfusion
Neuroinflammation
Activation of Microglia
Degradation of the Blood-Brain Barrier
Endothelial Dysfunction
Neuronal Network Alterations
Neurotransmitter Imbalances
Acetylcholine Depletion
Monoamine (Dopamine, Norepinephrine, and Serotonin) Depletion
Oxidative Stress
Disturbance of Circadian Integrity
Intensive Care Unit-Associated Delirium is Associated with Structural Changes in the Brain
Magnetic Resonance Imaging Studies Note a Relationship Between the Duration of Intensive Care Unit-Associated Delirium and Cerebral Atrophy and Cerebral White Matter Disruption [MEDLINE] [MEDLINE]
Diagnosis
Delirium Scoring Scales
Confusion Assessment Method for the Intensive Care Unit (CAM-ICU)
CAM-ICU Can Be Used as a Screening Tool for Delirium in the ICU (Crit Care, 2012) [MEDLINE]
Scoring System: positive or negative according to the presence or absence of criteria in a patient who is sufficiently awake (RASS −3 or more)
Acute Change from Mental Status at Baseline or Fluctuating Mental Status During the Past 24 hrs: must be true to be positive
More than 2 Errors on a 10Point Test of Attention to Voice or Pictures: must be true to be positive
If the RASS is Not 0 and the Above Two Criteria are Positive, the Patient is Delirious
If the RASS is 0 and the Above Two Criteria are Positive, Test for Disorganized Thinking Using 4 Yes/No Questions and a 2Step Command: >1 error means the patient is delirious; ≤1 error excludes delirium
Intensive Care Delirium Screening Checklist (ICDSC)
Scoring System: a score of ≥4 is positive for delirium (score 1-3: “subsyndromal delirium”) -> patient must show at least a response to mild-moderate stimulation
Anything Other than Normal Wakefulness
Disorientation
Disturbance in Sleep or Wake Cycle
Fluctuation in Symptoms
Hallucination
Inappropriate Speech/Mood
Inattention
Psychomotor Agitation
Recommendations (Clinical Practice Guidelines for the Management of Pain, Agitation, and Delirium in Adult Patients in the Intensive Care Unit; Critical Care Med, 2013) [MEDLINE]
Routine Monitoring for the Detection of Delirium is Recommended in Adult ICU Patients (Grade +1B Recommendation)
Routine Monitoring is Feasible in Clinical Practice (Grade B Recommendation)
Confusion Assessment Method for the ICU (CAM-ICU) and the Intensive Care Delirium Screening Checklist (ICDSC) are the Most Valid and Reliable Delirium Monitoring tools in Adult ICU Patients (Grade A Recommendation)
Clinical Manifestations
General Comments
Clinical Subtypes (Based on Psychomotor Alterations)
Hypoactive Subtype: most frequent subtype
Hypokinesia
Decreased Speech
Hyperactive Subtype
Hyperkinesia: restlessness, agitation
Autonomic Features (Tachycardia, Hyperventilation) are Common and May Result in Undesirable Physiologic Consequences (Such as Increased Myocardial Demand, etc)
This Type is Classically Associated with Alcohol Withdrawal (see Ethanol)
Mixed Motor subtype
Diurnal Variation in Symptoms
The Severity of Delirium Often Fluctuates During the Course of the Day with Nocturnal Restlessness (“Sundowning”) and Daytime Somnolence
Consequences of Intensive Care Unit-Associated Delirium (Especially in Mechanically Ventilated Patients)
Development of Long-Term Cognitive Impairment
Clinical Studies
Review Citing an Association Between Delirium in the ICU and Subsequent Cognitive Impairment (Neuropsychol Rev, 2004) [MEDLINE]
Study of the Impact of the Duration of Delirium in Mechanically Ventilated Medical ICU Patients (Crit Care Med, 2010) [MEDLINE]
Mean Age: 61 y/o
Longer Duration of Delirium was Associated with Increased Long-Term Cognitive Impairment
Duration of Mechanical Ventilation was Not Associated with Long-Term Cognitive Impairment
Study of the Impact of Delirium in Patients with Severe Sepsis (JAMA, 2010) [MEDLINE]
Mean Age of Survivors: 76.9 y/o
Severe Sepsis was Associated with Persistent and New Cognitive Impairment and Functional Disability in Survivors
BRAIN-ICU Study of Patients with Respiratory Failure or Shock in the Medical/Surgical ICU (NEJM, 2013) [MEDLINE]: n = 821)
Delirium Developed in 74% of Cases During Hospital Stay
Outcomes At 3 Months
40% of Patients Had Impaired Global Cognition Scores that Were 1.5 SD Below the Population Mean, Similar to Scores for Patients with Moderate Traumatic Brain Injury
26% of Patients Had Scores 2 SD Below the Population Mean (similar to scores for patients with Mild Alzheimer’s Disease
Outcomes At 12 Months
Similar Persistent Cognitive Dysfunction Occurs as in Those with Moderate Traumatic Brain Injury
Similar Persistent Cognitive Dysfunction Occurs as in Those with Mild Alzheimer’s Disease
Impact of Duration of Delirium
Longer Duration of Delirium was Significantly Associated with Worse Global Cognition at 3 and 12 Months and Worse Executive Function at 3 and 12 Months
Impact of Sedative Use
Use of Sedatives/Analgesics Were Not Associated with Cognitive Impairment at 3 and 12 Months
Cognitive Dysfunction was Also Independent of Age, Pre-Existing Cognitive Impairment, Presence or Severity of Coexisting Conditions, and Organ Failure During ICU Care
Delirium is Associated with Post-ICU Cognitive Impairment in Adult ICU Patients (Grade B Evidence) (Clinical Practice Guidelines for the Management of Pain, Agitation, and Delirium in Adult Patients in the Intensive Care Unit; Critical Care Med, 2013) [MEDLINE]
Delirium is Associated with the Later Development of Post-Traumatic Stress Disorder (PTSD) (Crit Care, 2007) [MEDLINE]
Functional Decline/Disability
Clinical Studies
Study of the Impact of Delirium in Patients with Severe Sepsis (JAMA, 2010) [MEDLINE]
Mean Age of Survivors: 76.9 y/o
Severe Sepsis was Associated with Persistent and New Cognitive Impairment and Functional Disability in Survivors
Higher Reintubation Rate
Clinical Studies
xxx
Increased Mortality Rate
Clinical Studies
Delirium is Associated with Increased Mortality Rate at 6 Months (JAMA, 2004) [MEDLINE]
ICU Delirium is Associated with 1-Year Mortality Rate in Patients >60 y/o (Am J Respir Crit Care Med, 2009) [MEDLINE]
Delirium is Associated with Increased Mortality Rate in Adult ICU Patients (Grade A Evidence) (Clinical Practice Guidelines for the Management of Pain, Agitation, and Delirium in Adult Patients in the Intensive Care Unit; Critical Care Med, 2013) [MEDLINE]
Japanese Epidemiology of Delirium in ICU (JEDI) Study (J Crit Care, 2014) [MEDLINE]: delirium during the ICU stay was not associated with higher mortality rates -> these data conflict with those from prior studies
Patient Removal of Urinary/Vascular Catheters
Clinical Studies
xxx
Prolonged ICU and Hospital Length of Stay
Clinical Studies
Delirium is Associated with Increased Hospital Length of Stay in Mechanically Ventilated ICU Patients (JAMA, 2004) [MEDLINE]
ICU Delirium is Associated with Increased Hospital Length of Stay (Crit Care Med, 2005) [MEDLINE]
Delirium is Associated with Increased ICU and Hospital Length of Stay in Adult ICU Patients (Grade A Evidence) (Clinical Practice Guidelines for the Management of Pain, Agitation, and Delirium in Adult Patients in the Intensive Care Unit; Critical Care Med, 2013) [MEDLINE]
Self-Extubation
Clinical Studies
xxx
Prevention of Delirium
Based on Synopsis of the National Institute for Health and Clinical Excellence Guideline for Prevention of Delirium (Ann Intern Med, 2011) [MEDLINE]
Address Cognitive Impairment or Disorientation
Ensure That a 24-hr Clock and a Calendar are Easily Visible to the Patient
Facilitate Regular Visits from Family/Friends
Orient Person to their Location, Who They Are, and What Your Role Is
Provide Appropriate Lighting and Clear Signage
Use Cognitively Stimulating Activities: reminiscence, etc
Assess Medication List for Number and Type of Medications
Avoid Physical Restraints: if possible
Ensure that Persons at Risk for Delirium are Cared for by a Team of Health Care Professionals Who are Familiar with the Person at Aisk
Avoid Moving Persons Within and Between Wards or Rooms: unless absolutely necessary
Multicomponent, Individualized Intervention Should be Delivered by a Multidisciplinary Team Trained and Competent in Delirium Prevention
Optimize Nutritional Status
Insert Dentures
Optimize Pain Management
Assess for Nonverbal Signs of Pain: particularly in patients with impaired ommunication
Institute Appropriate Pain Management
Promote Good Sleep Hygiene
Avoid Nursing or Medical Procedures During Sleeping Hours
Reduce Nighttime Noise
Schedule Medication Rounds to Avoid Disturbing Sleep
Utilize a Tailored, Multicomponent Intervention Package
Within 24 hrs of Hospitalization, Assess Persons at Risk for Delirium Risk Factors: provide a multicomponent, individualized intervention
Specific Prevention Measures
General Comments
Clinical Efficacy
Systematic Review of Pharmalogic Prevention and Treatment of Delirium in the ICU (J Crit Care, 2015) [MEDLINE]
The Use of Anti-Psychotics for Surgical Patients and Dexmedetomidine for Mechanically Ventilated Patients May Decrease the Incidence of Delirium in the ICU
However, None of the Studied Agents That Were Used for Delirium Treatment Improved Major Clinical Outcomes (Including Mortality)
MENDS Trial of Dexmedetomidine in Mechanically Ventilated Patients (JAMA, 2007) [MEDLINE]
Dexmedetomidine Increased the Number of Days Alive without Delirium/Coma and Achieved More Time at the Targeted Level of Sedation, as Compared to Lorazepam Infusion
Trial Comparing Sedation with Dexmedetomidine vs Benzodiazepines for Sedation in the ICU (JAMA, 2009) [MEDLINE]
At Comparable Sedation Levels, Dexmedetomidine Decreased the Incidence of Delirium and Ventilator Says, as Compared to Benzodiazepines
MIDEX and PRODEX Trials: Dexmedetomidine (Precedex) Compared to Midazolam (Versed) and Propofol (Diprivan) (JAMA, 2012) [MEDLINE]: data from randomized MIDEX (Midazolam vs. Dexmedetomidine) and PRODEX (Propofol vs. Dexmedetomidine) trials
Dexmedetomidine was Equivalent in Maintaining Light-Moderate Sedation
Dexmedetomidine Decreased the Duration of Mechanical Ventilation, as Compared to Midazolam (But Not When Compared to Propofol)
Dexmedetomidine Improved Patients’ Ability to Communicate Pain, as Compared with Midazolam and Propofol
Dexmedetomidine Demonstrated More Adverse Effects (Bradycardia/Hypotension), as Compared with Midazolam and Propofol
Rates of Anxiety/Agitation/Delirium were Lower with Dexmedetomidine than with Propofol, But the Rates were the Same Between Dexmedetomidine and Midazolam: CAM-ICU delirium rates assessed 48 hrs after sedation was stopped showed no differences between the groups
In the First 24 hrs of PRODEX Trial, Discontinuation of Dexmedetomidine was More Frequent Due to Lack of Efficacy: this suggests that adequate sedation may not be possible in all patients with dexmedetomidine alone (and it is likely that dexmedetomidine is not equivalent to propofol)
Dexmedetomidine (Precedex) to Lessen ICU Agitation (DahLIA) Trial (JAMA, 2016) [MEDLINE]: dexmedetomidine compared to placebo in agitated delirium in mechanically-ventilated patients in the ICU
Dexmedetomidine Increased Ventilator-Free Hours at 7 Days, as Compared to Usual Care
Dexmedetomidine Decreased Time to Extubation and Accelerated Resolution of Delirium
Early Mobilization in the Intensive Care Unit
Clinical Efficacy
Randomized Controlled Trial of Early Physical Therapy and Occupational Therapy in Mechanically Ventilated Patients in the ICU (Lancet, 2009) [MEDLINE]
Early Mobilization Decreased Duration of Delirium
Early Mobilization Improved Functional Outcome at Hospital Discharge
Trial of Haloperidol in Patients Undergoing Hip Fracture Surgery (J Am Geriatr Soc, 2005) [MEDLINE]
Low-Dose Haloperidol Did Not Decrease the Incidence of Post-Operative Delirium, But Did Improve the Severity and Duration of the Delirium and Decreased the Hospital Length of Stay
Trial of Haloperidol Prophylaxis in Elderly Patients Admitted to the ICU After Non-Cardiac Surgery (Crit Care Med, 2012) [MEDLINE]
Short-Term Prophylactic Low-Dose Intravenous Haloperidol Significantly Decreased the Incidence of Post-Operative Delirium
Dutch REDUCE Double-Blind, Placebo-Controlled Randomized Trial of Prophylactic Haloperidol in Patients at High-Risk for Delirium in the Intensive Care Unit ( JAMA, 2018) [MEDLINE]: n = 1789 (with 90-day follow-up)
Prophylactic Haloperidol Did Not Improve 28-Day Mortality in Patients at High-Risk for Delirium in the Intensive Care Unit
Systematic Review and Meta-Analysis of the Use of Antipsychotics in the Prevention and Treatment of Delirium in Hospitalized Patients (J Am Geriatr Soc, 2016) [MEDLINE]” n = 19 studies
In 7 Studies Comparing Antipsychotics vs Placebo or No Treatment for the Prevention of Delirium After Surgery, There was No Significant Effect on Delirium Incidence (OR = 0.56, 95% CI = 0.23-1.34, I(2) = 93%)
Using Data Reported from All 19 Studies, Antipsychotic Use was Not Associated with Any Change in Delirium Duration, Severity, or Hospital or ICU Length of Stay, with High Heterogeneity Among the Studies
No Association with Mortality was Detected (OR = 0.90, 95% CI = 0.62-1.29, I(2) = 0%)
Current Evidence Does Not Support the Use of Antipsychotics for the Prevention or Treatment of Delirium
Systematic Review of the Use of Antipsychotics for the Prevention of Delirium in Hospitalized Patients (Ann Intern Med, 2019 [MEDLINE]: n = 14 randomized controlled trials
For Haloperidol vs Placebo, There Were No Differences in Delirium Incidence or Duration, Hospital Length of Stay (High Strength of Evidence, and Mortality
Little or No Evidence was Found to Determine the Effect of Haloperidol on Cognitive Function, Delirium Severity (Insufficient Strength of Evidence), Inappropriate Continuation, and Sedation (Insufficient Strength of Evidence)
There is Limited Evidence that Second-Generation Antipsychotics May Decrease the Incidence of Delirium in the Postoperative Settings
There is Little Evidence that Short-Term Use of Antipsychotics was Associated with Neurologic Harm
In Some of the Trials, Potentially Harmful Cardiac Effects Occurred More Frequently with Antipsychotic Use
Trial of Ketamine Prophylaxis During Anesthetic Induction (with Fentanyl and Etomidate) for Cardiac Surgery with Cardiopulmonary Bypass (J Cardiothorac Vasc Anesth, 2009) [MEDLINE]
Ketamine Significantly Decreased the Incidence of Post-Operative Delirium and C-Reactive Protein Levels
Trial of Risperidone After Cardiac Surgery (Anaesth Intensive Care, 2007) [MEDLINE]
Single Dose of Risperidone Administered Soon after Cardiac Surgery with Cardiopulmonary Bypass Decreased the Incidence of Post-Operative Delirium
Systematic Review of the Use of Antipsychotics for the Prevention of Delirium in Hospitalized Patients (Ann Intern Med, 2019 [MEDLINE]: n = 14 randomized controlled trials
For Haloperidol vs Placebo, There Were No Differences in Delirium Incidence or Duration, Hospital Length of Stay (High Strength of Evidence, and Mortality
Little or No Evidence was Found to Determine the Effect of Haloperidol on Cognitive Function, Delirium Severity (Insufficient Strength of Evidence), Inappropriate Continuation, and Sedation (Insufficient Strength of Evidence)
There is Limited Evidence that Second-Generation Antipsychotics May Decrease the Incidence of Delirium in the Postoperative Settings
There is Little Evidence that Short-Term Use of Antipsychotics was Associated with Neurologic Harm
In Some of the Trials, Potentially Harmful Cardiac Effects Occurred More Frequently with Antipsychotic Use
Randomized Trial of Rivastigmine to Prevent Post-Operative Delirium Following Cardiothoracic Surgery (Crit Care Med, 2009) [MEDLINE]
Oral Rivastigmine Did Not Prevent Post-Operative Delirium in Elderly Patients Undergoing Elective Cardiac Surgery with Cardiopulmonary Bypass: study had methodologic issues, which were noted by the authors
Dutch Trial of Rivastigmine in Critically Ill Patients >18 y/o with Delirium (Lancet, 2010) [MEDLINE]
Rivastigmine Increased the Duration of Delirium and Mortality Rate in Critically Ill Patients, as Compared to Usual Care and Haloperidol
Systematic Reviews/Meta-Analyses Examining the Clinical Impact of Delirium Prevention Strategies
Impact of Delirium Prevention Interventions on Mortality Rate
Clinical Efficacy
Systematic Review and Meta-Analysis of Pharmacologic/Non-Pharmacologic Interventions to Decrease Delirium in the ICU (Crit Care Med, 2014) [MEDLINE]
Interventions Decreased the Duration of Delirium, But Did Not Impact the Short-Term Mortality Rate
Impact of Delirium Prevention Interventions in Hospitalized Non-ICU Patients
Clinical Efficacy
Systematic Review of Delirium Prevention Interventions in Non-ICU Patients (Cochrane Database Syst Rev, 2016) [MEDLINE]
Strong Evidence Supporting Multi-Component Interventions to Prevent Delirium in Hospitalised Patients
No Evidence That Cholinesterase Inhibitors, Antipsychotic Medication, or Melatonin Decrease the Incidence of Delirium
Bispectral Index to Monitor and Control the Depth of Anesthesia Decreases the Incidence of Post-Operative Delirium: however, the role of drugs and other anaesthetic techniques to prevent delirium remains uncertain
Recommendations (Clinical Practice Guidelines for the Management of Pain, Agitation, and Delirium in Adult Patients in the Intensive Care Unit; Critical Care Med, 2013) [MEDLINE]
Promotion of Sleep is Recommended in Adult ICU Patients (Grade +1C Recommendation)
Optimization of Patient Environments Using Strategies to Control Light and Noise
Clustering Patient Care Activities
Decreasing Nocturnal Stimuli to Protect Patient Sleep Cycles
Early Mobilization of Adult ICU Patients is Recommended Whenever Feasible to Decrease the Incidence and Duration of Delirium (Grade +1B Recommendation)
No Data Indicate that Either Haloperidol or Atypical Anti-Psychotics Prevent Delirium in Adult ICU Patients (Grade -2C Recommendation)
No Data Indicate that Dexmedetomidine Prevents Delirium in Adult ICU Patients (Grade 0, C Recommendation)
No Specific Recommendations are Available for Using a Pharmacologic Delirium Prevention Protocol in Adult ICU Patients (Grade 0, C Recommendation): no data demonstrate that this reduces the incidence or duration of delirium
In Addition, No Specific Recommendations are Available for Using a Combined Pharmacologic and Non-Pharmacologic Delirium Prevention Protocol in Adult ICU Patients (Grade 0, C Recommendation): no data demonstrate that this reduces the incidence of delirium
No Specific Recommendations are Available for Specific Mechanical Ventilation Modes to Promote Sleep in Mechanically Ventilated Adult ICU Patients (Grade 0 Recommendation, No Evidence)
An Interdisciplinary ICU Team Should Be Employed (with Provider Education, Protocols/Order Sets, and Quality ICU Rounds Checklists to Facilitate the Use of Pain, Agitation, and Delirium Management Guidelines/Protocols in Adult ICU’s (Grade +1B Recommendation)
Treatment of Delirium
General Management
Maintenance of Patient Safety and Therapeutic Devices (Endotracheal Tube, Catheters, etc)
Avoidance of Falls
Prevention of Self-Extubation
Agents
General Comments
Clinical Efficacy
Systematic Review of Pharmalogic Prevention and Treatment of Delirium in the ICU J Crit Care, 2015) [MEDLINE]
The Use of Anti-Psychotics for Surgical Patients and Dexmedetomidine for Mechanically Ventilated Patients May Decrease the Incidence of Delirium in the ICU
However, None of the Studied Agents That Were Used for Delirium Treatment Improved Major Clinical Outcomes (Including Mortality)
Trial of Dexmedetomidine vs Haloperidol in Agitated Delirium in Mechanically Ventilated Patients (Crit Care, 2009) [MEDLINE]
Dexmedetomidine Decreased the Time to Extubation and ICU Length of Stay, As Compared to Haloperidol
Dexmedetomidine Decreased the Propofol Requirement
Dexmedetomidine (Precedex) to Lessen ICU Agitation (DahLIA) Trial (JAMA, 2016) [MEDLINE]: dexmedetomidine compared to placebo in agitated delirium in mechanically-ventilated patients in the ICU
Dexmedetomidine Increased Ventilator-Free Hours at 7 Days, as Compared to Usual Care
Dexmedetomidine Decreased Time to Extubation and Accelerated Resolution of Delirium
Dopamine receptor antagonist that inhibits dopamine neurotransmission and results in a sedative effect
Adverse Effects: cognitive numbness and dysphoria in 40% of patients, seizures, extrapyramidal symptoms, QT prolongation
Clinical Efficacy
Trial of Olanzapine vs Haloperidol in Delirium in the Intensive Care Unit Setting (Intensive Care Med, 2004) [MEDLINE]
Delirium Index and Benzodiazepine Administration Decreased Over Time in Both Groups: clinical improvement was similar in both groups
No Side Effects Were Noted in the Olanzapine Group, Whereas the Haloperidol Group Had Extrapyramidal Side Effects
Systematic Review of Anti-Psychotics for Delirium (Cochrane Database Syst Rev, 2007) [MEDLINE]
No Evidence that Haloperidol (at Low Dosage) Has Different Efficacy in the Management of Delirium or Greater Frequency of Adverse Effects than Olanzapine and Risperidone
High-Dose Haloperidol Has a Higher Incidence of Adverse Effects (Mainly Parkinsonism) than the Atypical Anti-Psychotics
Low-Dose Haloperidol May be Effective in Decreasing the Degree and Duration of Delirium in Post-Operative Patients, as Compared to Placebo
Trial of Dexmedetomidine vs Haloperidol in Agitated Delirium in Mechanically Ventilated Patients (Crit Care, 2009) [MEDLINE]
Dexmedetomidine Decreased the Time to Extubation and ICU Length of Stay, As Compared to Haloperidol
Dexmedetomidine Decreased the Propofol Requirement
MIND Trial of Haloperidol, Ziprasidone, or Placebo in Delirium in the Intensive Care Unit (Crit Care Med, 2010) [MEDLINE]
Haloperidol and Ziprasidone Did not Improve the Number of Days Alive Without Delirium or Coma, Nor Did They Increase Adverse Outcomes
Hope-ICU Trial of Haloperidol in Critically Ill Patients (Lancet Respir Med, 2013) [MEDLINE]: double-blind, placebo-controlled randomised trial of haloperidol 2-5 mg vs normal saline placebo IV q8h, irrespective of coma or delirium status
No Evidence that Haloperidol Modified the Duration of Delirium in Critically Ill Patients: although haloperidol is safe in ICU delirium, pending the results of trials in progress, the use of IV haloperidol should be reserved for short-term management of acute agitation
Systematic Review and Meta-Analysis of the Use of Antipsychotics in the Prevention and Treatment of Delirium in Hospitalized Patients (J Am Geriatr Soc, 2016) [MEDLINE]” n = 19 studies
In 7 Studies Comparing Antipsychotics vs Placebo or No Treatment for the Prevention of Delirium After Surgery, There was No Significant Effect on Delirium Incidence (OR = 0.56, 95% CI = 0.23-1.34, I(2) = 93%)
Using Data Reported from All 19 Studies, Antipsychotic Use was Not Associated with Any Change in Delirium Duration, Severity, or Hospital or ICU Length of Stay, with High Heterogeneity Among the Studies
No Association with Mortality was Detected (OR = 0.90, 95% CI = 0.62-1.29, I(2) = 0%)
Current Evidence Does Not Support the Use of Antipsychotics for the Prevention or Treatment of Delirium
MIND-USA Trial of Haloperidol and Ziprasidone in the Treatment of Delirium in Critically Ill Patients (NEJM, 2018) [MEDLINE]: n = 566
Patient Population: 89% had hypoactive delirium and 11% had hyperactive delirium
The Median Duration of Exposure to a Trial Drug or Placebo was 4 Days (Interquartile Range: 3-7 Days)
The Median Number of Days Alive without Delirium or Coma was 8.5 (95% CI: 5.6-9.9) in the Placebo Group, 7.9 (95% CI: 4.4-9.6) in the Haloperidol Group, and 8.7 (95% CI: 5.9-10.0) in the Ziprasidone Group (P=0.26 for Overall Effect Across Trial Groups)
In Patients with Acute Respiratory Failure or Shock and Hypoactive/Hyperactive Delirium in the ICU, the Use of Haloperidol or Ziprasidone, Did Not Significantly Alter the Duration of Delirium, as Compared to Placebo
Systematic Review of the Use of Antipsychotics for Treatment of Delirium in Hospitalized Adults (Ann Intern Med, 2019) [MEDLINE]” n = 16 RCT’s and 10 observational studies
Across 16 RCT’s and 10 Observational Studies, For Second-Generation Antipsychotics vs Placebo and Haloperidol vs Placebo, There was no Difference in Sedation Status Low and Moderate Strength of Evidence), Duration of Delirium, Hospital Length os Stay (Moderate Strength of Evidence), or Mortality Rate
There was No Difference in Delirium Severity (Moderate Strength of Evidence) and Cognitive Functioning (Low Strength of Evidence) for Haloperidol vs Second-Generation Antipsychotics, with Insufficient or No Evidence for Antipsychotics vs Placebo*
For Direct Comparisons of Different Second-Genration Antipsychotics, There was No Difference in Mortality and Insufficient or No Evidence for Multiple Other Outcomes
There was Little Evidence Demonstrating Neurologic Harm Associated with Short-Term Antipsychotic Use for the Treatment of Delirium in Adult Inpatients, But Potentially Harmful Cardiac Effects Tended to Occur More Frequently
Heterogeneity was Present in Terms of Dose and Administration Route of Antipsychotics, Outcomes, and Measurement Instruments
Danish Multicenter, Randomized, Placebo-Controlled AID-ICU Trial of Haloperidol Use in the Treatment of Delirium in Adults Patients in the Intensive Care Unit (NEJM, 2022) [MEDLINE]: n = 987 included in final analysis
At 90 Days, the Mean Number of Days Alive and Out of the Hospital was 35.8 (95% CI: 32.9-38.6) in the Haloperidol Group and 32.9 (95% CI: 29.9-35.8) in the Placebo Group
Adjusted Mean Difference was 2.9 Days (95% CI: -1.2 to 7.0) (P = 0.22)
Mortality at 90 Days was 36.3% in the Haloperidol Group and 43.3% in the Placebo Group
Adjusted Absolute Difference was -6.9 Percentage Points (95% CI: -13.0 to -0.6)
Serious Adverse Reactions Occurred in 11 Patients in the Haloperidol Group and in 9 Patients in the Placebo Group
Conclusion
In ICU Patients with Delirium, Haloperidol Did Not Lead to a Significantly Greater Number of Days Alive and Out of the Hospital at 90 Days than Placebo
Pharmacology: second-generation antipsychotic olanzapine has been advocated because of its more favorable side effect profile, oral bioavailablity and lack of active metabolites
Clinical Efficacy
Trial of Olanzapine vs Haloperidol in Delirium in the Intensive Care Unit Setting (Intensive Care Med, 2004) [MEDLINE]
Delirium Index and Benzodiazepine Administration Decreased Over Time in Both Groups: clinical improvement was similar in both groups
No Side Effects Were Noted in the Olanzapine Group, Whereas the Haloperidol Group Had Extrapyramidal Side Effects
Systematic Review of Anti-Psychotics for Delirium (Cochrane Database Syst Rev, 2007) [MEDLINE]
No Evidence that Haloperidol (at Low Dosage) Has Different Efficacy in the Management of Delirium or Greater Frequency of Adverse Effects than Olanzapine and Risperidone
High-Dose Haloperidol Has a Higher Incidence of Adverse Effects (Mainly Parkinsonism) than the Atypical Anti-Psychotics
Low-Dose Haloperidol May be Effective in Decreasing the Degree and Duration of Delirium in Post-Operative Patients, as Compared to Placebo
Systematic Review and Meta-Analysis of the Use of Antipsychotics in the Prevention and Treatment of Delirium in Hospitalized Patients (J Am Geriatr Soc, 2016) [MEDLINE]” n = 19 studies
In 7 Studies Comparing Antipsychotics vs Placebo or No Treatment for the Prevention of Delirium After Surgery, There was No Significant Effect on Delirium Incidence (OR = 0.56, 95% CI = 0.23-1.34, I(2) = 93%)
Using Data Reported from All 19 Studies, Antipsychotic Use was Not Associated with Any Change in Delirium Duration, Severity, or Hospital or ICU Length of Stay, with High Heterogeneity Among the Studies
No Association with Mortality was Detected (OR = 0.90, 95% CI = 0.62-1.29, I(2) = 0%)
Current Evidence Does Not Support the Use of Antipsychotics for the Prevention or Treatment of Delirium
Systematic Review of the Use of Antipsychotics for Treatment of Delirium in Hospitalized Adults (Ann Intern Med, 2019) [MEDLINE]” n = 16 RCT’s and 10 observational studies
Across 16 RCT’s and 10 Observational Studies, For Second-Generation Antipsychotics vs Placebo and Haloperidol vs Placebo, There was no Difference in Sedation Status Low and Moderate Strength of Evidence), Duration of Delirium, Hospital Length os Stay (Moderate Strength of Evidence), or Mortality Rate
There was No Difference in Delirium Severity (Moderate Strength of Evidence) and Cognitive Functioning (Low Strength of Evidence) for Haloperidol vs Second-Generation Antipsychotics, with Insufficient or No Evidence for Antipsychotics vs Placebo*
For Direct Comparisons of Different Second-Genration Antipsychotics, There was No Difference in Mortality and Insufficient or No Evidence for Multiple Other Outcomes
There was Little Evidence Demonstrating Neurologic Harm Associated with Short-Term Antipsychotic Use for the Treatment of Delirium in Adult Inpatients, But Potentially Harmful Cardiac Effects Tended to Occur More Frequently
Heterogeneity was Present in Terms of Dose and Administration Route of Antipsychotics, Outcomes, and Measurement Instruments
Adverse Effects: almost all psychotropic drugs used for delirium may have an impact on QTc interval prolongation, but quetiapine typically has less of an impact than haloperidol
Clinical Efficacy
Trial of Quetiapine (Added to Haloperidol PRN) in Established Delirium in Critically Ill Patients (Crit Care Med, 2010) [MEDLINE]
Quetiapine (Added to Haloperidol PRN) Decreased the Time to Resolution of Delirium, Resulted in Less Agitation, and Resulted in Greater Rates of Transfer to Home or Rehabilitation
No Differences in the Rates of QT Prolongation Between the Groups, Although the Quetiapine Group was More Somnolent
Systematic Review and Meta-Analysis of the Use of Antipsychotics in the Prevention and Treatment of Delirium in Hospitalized Patients (J Am Geriatr Soc, 2016) [MEDLINE]” n = 19 studies
In 7 Studies Comparing Antipsychotics vs Placebo or No Treatment for the Prevention of Delirium After Surgery, There was No Significant Effect on Delirium Incidence (OR = 0.56, 95% CI = 0.23-1.34, I(2) = 93%)
Using Data Reported from All 19 Studies, Antipsychotic Use was Not Associated with Any Change in Delirium Duration, Severity, or Hospital or ICU Length of Stay, with High Heterogeneity Among the Studies
No Association with Mortality was Detected (OR = 0.90, 95% CI = 0.62-1.29, I(2) = 0%)
Current Evidence Does Not Support the Use of Antipsychotics for the Prevention or Treatment of Delirium
Systematic Review of the Use of Antipsychotics for Treatment of Delirium in Hospitalized Adults (Ann Intern Med, 2019) [MEDLINE]” n = 16 RCT’s and 10 observational studies
Across 16 RCT’s and 10 Observational Studies, For Second-Generation Antipsychotics vs Placebo and Haloperidol vs Placebo, There was no Difference in Sedation Status Low and Moderate Strength of Evidence), Duration of Delirium, Hospital Length os Stay (Moderate Strength of Evidence), or Mortality Rate
There was No Difference in Delirium Severity (Moderate Strength of Evidence) and Cognitive Functioning (Low Strength of Evidence) for Haloperidol vs Second-Generation Antipsychotics, with Insufficient or No Evidence for Antipsychotics vs Placebo*
For Direct Comparisons of Different Second-Genration Antipsychotics, There was No Difference in Mortality and Insufficient or No Evidence for Multiple Other Outcomes
There was Little Evidence Demonstrating Neurologic Harm Associated with Short-Term Antipsychotic Use for the Treatment of Delirium in Adult Inpatients, But Potentially Harmful Cardiac Effects Tended to Occur More Frequently
Heterogeneity was Present in Terms of Dose and Administration Route of Antipsychotics, Outcomes, and Measurement Instruments
Systematic Review of Antipsychotics for Delirium (Cochrane Database Syst Rev, 2007) [MEDLINE]
No Evidence that Haloperidol (at Low Dosage) Has Different Efficacy in the Management of Delirium or Greater Frequency of Adverse Effects than Olanzapine and Risperidone
High-Dose Haloperidol Has a Higher Incidence of Adverse Effects (Mainly Parkinsonism) than the Atypical Anti-Psychotics
Low-Dose Haloperidol May be Effective in Decreasing the Degree and Duration of Delirium in Post-Operative Patients, as Compared to Placebo
Systematic Review of the Use of Antipsychotics for Treatment of Delirium in Hospitalized Adults (Ann Intern Med, 2019) [MEDLINE]” n = 16 RCT’s and 10 observational studies
Across 16 RCT’s and 10 Observational Studies, For Second-Generation Antipsychotics vs Placebo and Haloperidol vs Placebo, There was no Difference in Sedation Status Low and Moderate Strength of Evidence), Duration of Delirium, Hospital Length os Stay (Moderate Strength of Evidence), or Mortality Rate
There was No Difference in Delirium Severity (Moderate Strength of Evidence) and Cognitive Functioning (Low Strength of Evidence) for Haloperidol vs Second-Generation Antipsychotics, with Insufficient or No Evidence for Antipsychotics vs Placebo*
For Direct Comparisons of Different Second-Genration Antipsychotics, There was No Difference in Mortality and Insufficient or No Evidence for Multiple Other Outcomes
There was Little Evidence Demonstrating Neurologic Harm Associated with Short-Term Antipsychotic Use for the Treatment of Delirium in Adult Inpatients, But Potentially Harmful Cardiac Effects Tended to Occur More Frequently
Heterogeneity was Present in Terms of Dose and Administration Route of Antipsychotics, Outcomes, and Measurement Instruments
MIND Trial of Haloperidol, Ziprasidone, or Placebo in Delirium in the Intensive Care Unit (Crit Care Med, 2010) [MEDLINE]
Haloperidol and Ziprasidone Did not Improve the Number of Days Alive Without Delirium or Coma, Nor Did They Increase Adverse Outcomes
Systematic Review and Meta-Analysis of the Use of Antipsychotics in the Prevention and Treatment of Delirium in Hospitalized Patients (J Am Geriatr Soc, 2016) [MEDLINE]” n = 19 studies
In 7 Studies Comparing Antipsychotics vs Placebo or No Treatment for the Prevention of Delirium After Surgery, There was No Significant Effect on Delirium Incidence (OR = 0.56, 95% CI = 0.23-1.34, I(2) = 93%)
Using Data Reported from All 19 Studies, Antipsychotic Use was Not Associated with Any Change in Delirium Duration, Severity, or Hospital or ICU Length of Stay, with High Heterogeneity Among the Studies
No Association with Mortality was Detected (OR = 0.90, 95% CI = 0.62-1.29, I(2) = 0%)
Current Evidence Does Not Support the Use of Antipsychotics for the Prevention or Treatment of Delirium
MIND-USA Trial of Haloperidol and Ziprasidone in the Treatment of Delirium in Critically Ill Patients (NEJM, 2018) [MEDLINE]: n = 566
Patient Population: 89% had hypoactive delirium and 11% had hyperactive delirium
The Median Duration of Exposure to a Trial Drug or Placebo was 4 Days (Interquartile Range: 3-7 Days)
The Median Number of Days Alive without Delirium or Coma was 8.5 (95% CI: 5.6-9.9) in the Placebo Group, 7.9 (95% CI: 4.4-9.6) in the Haloperidol Group, and 8.7 (95% CI: 5.9-10.0) in the Ziprasidone Group (P=0.26 for Overall Effect Across Trial Groups)
In Patients with Acute Respiratory Failure or Shock and Hypoactive/Hyperactive Delirium in the ICU, the Use of Haloperidol or Ziprasidone, Did Not Significantly Alter the Duration of Delirium, as Compared to Placebo
Systematic Review of the Use of Antipsychotics for Treatment of Delirium in Hospitalized Adults (Ann Intern Med, 2019) [MEDLINE]” n = 16 RCT’s and 10 observational studies
Across 16 RCT’s and 10 Observational Studies, For Second-Generation Antipsychotics vs Placebo and Haloperidol vs Placebo, There was no Difference in Sedation Status Low and Moderate Strength of Evidence), Duration of Delirium, Hospital Length os Stay (Moderate Strength of Evidence), or Mortality Rate
There was No Difference in Delirium Severity (Moderate Strength of Evidence) and Cognitive Functioning (Low Strength of Evidence) for Haloperidol vs Second-Generation Antipsychotics, with Insufficient or No Evidence for Antipsychotics vs Placebo*
For Direct Comparisons of Different Second-Genration Antipsychotics, There was No Difference in Mortality and Insufficient or No Evidence for Multiple Other Outcomes
There was Little Evidence Demonstrating Neurologic Harm Associated with Short-Term Antipsychotic Use for the Treatment of Delirium in Adult Inpatients, But Potentially Harmful Cardiac Effects Tended to Occur More Frequently
Heterogeneity was Present in Terms of Dose and Administration Route of Antipsychotics, Outcomes, and Measurement Instruments
Nonpharmacologic Therapies
Review of Nonpharmacologic Music Therapy for the Treatment of Delirium (Chest, 2022) [MEDLINE]
Sedation is an essential component of treatment for some patients admitted to the ICU, but it carries a risk of sedation-related delirium
Sedation-related delirium is associated with higher mortality and increased length of stay, but pharmacologic treatments for delirium can lead to oversedation or other adverse effects
Therefore, nonpharmacologic treatments are recommended in the literature; however, these recommendations are quite general and do not provide structured interventions
To establish a structured nonpharmacologic intervention that could improve indications of delirium after sedation, we combined evidence-based interventions including recordings of sensory-rich stories told by the patient’s family and patient-specific music into our novel positive stimulation for medically sedated patients (PSMSP) protocol
The positive listening stimulation playlist organized by a board-certified music therapist (MT-BC) within the PSMSP protocol can be used in carefully monitored sessions with the MT-BC potentially to decrease agitation and stabilize arousal, as well as being played by nursing staff throughout the patient’s recovery from sedation
Further controlled studies will be necessary, but the PSMSP protocol has the potential to reduce agitation and increase arousal during listening, as highlighted by the case of a patient recovering from sedation during treatment for COVID-19 pneumonia
It is important for the entire critical care team to be aware of nonpharmacologic treatments like PSMSP that are available for delirium mitigation so that, where applicable, these therapies can be incorporated into the patient’s treatment regimen
Recommendations (Clinical Practice Guidelines for the Management of Pain, Agitation, and Delirium in Adult Patients in the Intensive Care Unit; Critical Care Med, 2013) [MEDLINE]
No Published Evidence that Haloperidol Decreases the Duration of Delirium in Adult ICU Patients (No Evidence)
Atypical Anti-Psychotics May Decrease the Duration of Delirium in Adult ICU Patients (Grade C Recommendation)
Rivastigmine is Not Recommended to Decrease the Duration of Delirium in Adult ICU Patients (Grade -1B Recommendation)
Atypical Anti-Psychotics are Not Recommended in Patients at Risk for Torsade (Grade -2C Recommendation
Patients with Baseline QT Prolongation
Patients with History of Torsade
Patients Receiving Other QT Prolonging Medications
In Patients with Delirium Unrelated to Ethanol or Benzodiazepine Withdrawal, Dexmedetomidine is Preferred Over Benzodiazepines for Sedation to Decrease the Duration of Delirium (Grade +B Recommendation)
Prognosis
Clinical Data
BRAIN-ICU Study of Patients with Respiratory Failure or Shock in the Medical/Surgical ICU (NEJM, 2013) [MEDLINE]: n = 821)
Delirium Developed in 74% of Cases During Hospital Stay
Outcomes At 3 Months
40% of Patients Had Impaired Global Cognition Scores that Were 1.5 SD Below the Population Mean, Similar to Scores for Patients with Moderate Traumatic Brain Injury
26% of Patients Had Scores 2 SD Below the Population Mean (similar to scores for patients with Mild Alzheimer’s Disease
Outcomes At 12 Months
Similar Persistent Cognitive Dysfunction Occurs as in Those with Moderate Traumatic Brain Injury
Similar Persistent Cognitive Dysfunction Occurs as in Those with Mild Alzheimer’s Disease
Impact of Duration of Delirium
Longer Duration of Delirium was Significantly Associated with Worse Global Cognition at 3 and 12 Months and Worse Executive Function at 3 and 12 Months
Impact of Sedative Use
Use of Sedatives or Analgesics was Not Associated with Cognitive Impairment at 3 and 12 Months
Cognitive Dysfunction was Also Independent of Age, Pre-Existing Cognitive Impairment, Presence or Severity of Coexisting Conditions, and Organ Failure During ICU Care
Systematic Review of Delirium and Outcomes in Critically Ill Patients (BMJ, 2015) [MEDLINE]
Delirium was Identified in 5,280 of 16,595 (31.8%) Critically Ill Patients Reported in 42 Studies
When compared with control patients without delirium, patients with delirium had significantly higher mortality during admission (risk ratio 2.19, 94% confidence interval 1.78 to 2.70; P<0.001) as well as longer durations of mechanical ventilation and lengths of stay in the intensive care unit and in hospital (standard mean differences 1.79 (95% confidence interval 0.31 to 3.27; P<0.001), 1.38 (0.99 to 1.77; P<0.001), and 0.97 (0.61 to 1.33; P<0.001), respectively)
Available studies indicated an association between delirium and cognitive impairment after discharge
Association of Incident Delirium With Short-term Mortality in Adults With Critical Illness Receiving Mechanical Ventilation. JAMA Netw Open. 2022 Oct 3;5(10):e2235339. doi: 10.1001/jamanetworkopen.2022.35339 [MEDLINE]
Of 267 participants (median [IQR] age, 65.9 [57.4-75.1] years; 171 men [64.0%]; all of Taiwanese ethnicity), 149 patients (55.8%) developed delirium for a median (IQR) of 3.0 (1.0-5.0) days at some point during their first 14 days of ICU stay, and 105 patients (39.3%) had coma episodes also lasting for a median (IQR) of 3.0 (1.0-5.0) days
The 14-day and in-hospital mortality rates were 18.0% (48 patients) and 42.1% (112 of 266 patients [1 patient withdrew from the study]), respectively
The incidence and days of delirium were not associated with either 14-day mortality (incident delirium: adjusted hazard ratio [aHR], 1.37; 95% CI, 0.69-2.72; delirium by day: aHR, 1.00; 95% CI, 0.91-1.10) or in-hospital mortality (incident delirium: aHR, 1.00; 95% CI, 0.64-1.55; delirium by day: aHR, 1.02; 95% CI, 0.97-1.07), whereas days spent in coma were associated with an increased hazard of dying during a given 14-day period (aHR, 1.16; 95% CI, 1.10-1.22) and during hospitalization (aHR, 1.10; 95% CI, 1.06-1.14)
The number of delirium- and coma-free days was a protective factor; for each additional delirium- and coma-free days, the risk of dying during the 14-day period was reduced by 11% (aHR, 0.89; 95% CI, 0.84-0.94), and the risk of dying during hospitalization was reduced by 7% (aHR, 0.93; 95% CI, 0.90-0.97)
Incident delirium was associated with longer hospital stays (adjusted β = 10.80; 95% CI, 0.53-21.08) when compared with no incident delirium
Conclusions: In this study, despite prolonged LOS, ICU delirium was not associated with short-term mortality
However, delirium- and coma-free days were associated with a lower risk of dying, suggesting that future research and intervention implementation should refocus on maximizing delirium- and coma-free days to potentially improve the survival of patients receiving mechanical ventilation
References
General
www.icudelirium.org
The relationship of postoperative delirium with psychoactive medications. JAMA. 1994;272:1518-1522 [MEDLINE]
The use of continuous IV sedation is associated with prolongation of mechanical ventilation. Chest. 1998;114:541-548 [MEDLINE]
Causes of ICU psychosis: the environmental factors. Nurs Crit Care. 1999;4:22-26 [MEDLINE]
A multicomponent intervention to prevent delirium in hospitalized older patients. N Engl J Med. 1999;340:669-676 [MEDLINE]
Effect of a nursing-implemented sedation protocol on the duration of mechanical ventilation. Chest. 2000;117:809-818
Delirium in an intensive care unit: a study of risk factors. Intensive Care Med. 2001;27:1297-1304 [MEDLINE]
Elderly patients’ reports of physical restraint experiences in intensive care units. Am J Crit Care. 2001 May;10(3):168-71 [MEDLINE]
Evaluation of delirium in critically ill patients: validation of the Confusion Assessment Method for the Intensive Care Unit (CAM-ICU). Crit Care Med. 2001;29:1370-1379.
The association between delirium and cognitive decline: a review of the empirical literature. Neuropsychol Rev 2004; 14:87-98 [MEDLINE]
Delirium as a predictor of mortality in mechanically ventilated patients in the intensive care unit. JAMA 2004 Apr 14;291(14):1753-62 [MEDLINE]
Sleep disruption in critically ill patients—pharmacological considerations. Anaesthesia 2004;59(4):374–84 [MEDLINE]
Delirium: acute cognitive dysfunction in the critically ill. Curr Opin Crit Care 2005; 11(4):360-368 [MEDLINE]
Intensive care unit delirium is an independent predictor of longer hospital stay: a prospective analysis of 261 non-ventilated patients. Crit Care. 2005 Aug;9(4):R375-81. Epub 2005 Jun 1 [MEDLINE]
Risk factors for posttraumatic stress disorder symptoms following critical illness requiring mechanical ventilation: a prospective cohort study. Crit Care 2007;11:R28 [MEDLINE]
Incidence, risk factors and consequences of ICU delirium. Intensive Care Med. 2007;33:66-73 [MEDLINE]
Delirium in the acute care setting: characteristics, diagnosis and treatment. Crit Care Clin 2008;24:657-722 [MEDLINE]
Vanderbilt University Medical Center; Veterans Affairs TN Valley Research Education and Clinical Center (GRECC). Delirium overview. ICU Delirium and Cognitive Impairment Study Group: Brain Dysfunction in Critically Ill Patients Web site. https://www.icudelirium.org/delirium/Del%20overview.html. Published 2003. Updated 2008
Prevalence and risk factors for development of delirium in surgical and trauma ICU patients. J Trauma. 2008;65:34-41 [MEDLINE]
Delirium in the intensive care unit. Crit Care. 2008;12(suppl 3):S3 [MEDLINE]
Influence of physical restraint on unplanned extubation of adult intensive care patients: a case-control study. Am J Crit Care. 2008;17:408–415 [MEDLINE]
Days of delirium are associated with 1-year mortality in an older intensive care unit population. Am J Respir Crit Care Med 2009; 180:1092-1097 [MEDLINE]
Early physical and occupational therapy in mechanically ventilated, critically ill patients: a randomised controlled trial. Lancet 2009; 373:1874-1882 [MEDLINE]
Long-term cognitive impairment and functional disability among survivors of severe sepsis. JAMA 2010;304:1787-1794 [MEDLINE]
Delirium as a predictor of long-term cognitive impairment in survivors of critical illness. Crit Care Med 2010; 38:1513-1520 [MEDLINE]
Efficacy and safety of quetiapine in critically ill patients with delirium: a prospective, multicenter, randomized, double-blind, placebo-controlled pilot study. Crit Care Med 2010;38:419-27 [MEDLINE]
MIND Trial. Feasibility, efficacy, and safety of antipsychotics for intensive care unit delirium: the MIND randomized, placebo-controlled trial. Crit Care Med 2010;38: 428-37 [MEDLINE]
Synopsis of the National Institute for Health and Clinical Excellence Guideline for Prevention of Delirium. Ann Intern Med. 2011;154:746-751 [MEDLINE]
Delirium in the intensive care unit: A review. Neurol Clin 2011; 29:749-763 [MEDLINE]
The effect of earplugs during the night on the onset of delirium and sleep perception: A randomized controlled trial in intensive care patients. Crit Care 2012;16:R73 [MEDLINE]
The confusion assessment method for the intensive care unit (CAM-ICU) and intensive care delirium screening checklist (ICDSC) for the diagnosis of delirium: a systematic review and meta-analysis of clinical studies. Crit Care. 2012 Jul 3;16(4):R115. doi: 10.1186/cc11407 [MEDLINE]
Pharmacological and nonpharmacological management of delirium in critically ill patients. Neurotherapeutics 2012; 9:158-175 [MEDLINE]
Management of delirium in adult critically ill patients: an overview. J Pharm Pharm Sci. 2012;15:499–509 [MEDLINE]
The association between brain volumes, delirium duration, and cognitive outcomes in intensive care unit survivors: the VISIONS cohort magnetic resonance imaging study. Crit Care Med 2012;40: 2022-32 [MEDLINE]
The relationship between delirium duration, white matter integrity, and cognitive impairment in intensive care unit survivors as determined by diffusion tensor imaging: the VISIONS prospective cohort magnetic resonance imaging study. Crit Care Med 2012;40:2182-9 [MEDLINE]
The effect of a quality improvement intervention on perceived sleep quality and cognition in a medical ICU. Crit Care Med 2013;41:800-809 [MEDLINE]
Clinical practice guidelines for the management of pain, agitation and delirium in adult patients in the intensive care unit. Crit Care Med. 2013;41:263–306 [MEDLINE]
BRAIN-ICU Study. Long-term cognitive impairment after critical illness. N Engl J Med. 2013 Oct 3;369(14):1306-16. doi: 10.1056/NEJMoa1301372 [MEDLINE]
Preventing delirium in the intensive care unit. Crit Care Clin. 2013 Jan;29(1):51-65. doi: 10.1016/j.ccc.2012.10.007 [MEDLINE]
Effect of intravenous haloperidol on the duration of delirium and coma in critically ill patients (Hope-ICU): a randomised, double-blind, placebo-controlled trial. Lancet Respir Med. 2013 Sep;1(7):515-23. doi: 10.1016/S2213-2600(13)70166-8 [MEDLINE]
Corticosteroids and transition to delirium in patients with acute lung injury. Crit Care Med. 2014 Jun;42(6):1480-6. doi: 10.1097/CCM.0000000000000247 [MEDLINE]
Sedation and delirium in the intensive care unit. N Engl J Med. 2014;370:444–454 [MEDLINE]
JEDI Study. Delirium and coma evaluated in mechanically ventilated patients in the intensive care unit in Japan: a multi-institutional prospective observational study. J Crit Care. 2014 Jun;29(3):472.e1-5. doi: 10.1016/j.jcrc.2014.01.021. Epub 2014 Feb 3 [MEDLINE]
Randomized ICU trials do not demonstrate an association between interventions that reduce delirium duration and short-term mortality: a systematic review and meta-analysis. Crit Care Med. 2014 Jun;42(6):1442-54. doi: 10.1097/CCM.0000000000000224 [MEDLINE]
Predictors of physical restraint use in Canadian intensive care units. Crit Care. 2014;18(2):R46. doi: 10.1186/cc13789 [MEDLINE]
Risk factors for delirium after on-pump cardiac surgery: a systematic review. Crit Care. 2015 Sep 23;19:346. doi: 10.1186/s13054-015-1060-0 [MEDLINE]
Pharmacologic prevention and treatment of delirium in intensive care patients: A systematic review. J Crit Care. 2015 Aug;30(4):799-807. doi: 10.1016/j.jcrc.2015.04.005. Epub 2015 Apr 17 [MEDLINE]
Delirium in critically ill patients. Crit Care Clin. 2015 Jul;31(3):589-603. doi: 10.1016/j.ccc.2015.03.011. Epub 2015 May 4 [MEDLINE]
Systemic Corticosteroids And Transition To Delirium in Critically Ill Patients. Intensive Care Med Exp. 2015 Dec;3(Suppl 1):A30. doi: 10.1186/2197-425X-3-S1-A30 [MEDLINE]
Interventions for preventing delirium in hospitalised non-ICU patients. Cochrane Database Syst Rev. 2016 Mar 11;3:CD005563. doi: 10.1002/14651858.CD005563.pub3 [MEDLINE]
MENDS Trial. Effect of sedation with dexmedetomidine vs lorazepam on acute brain dysfunction in mechanically ventilated patients: the MENDS randomized controlled trial. JAMA 2007;298:2644-53 [MEDLINE]
Dexmedetomidine vs midazolam for sedation of critically ill patients: a randomized trial. JAMA 2009;301:489-9 [MEDLINE]
Dexmedetomidine vs. haloperidol in delirious, agitated, intubated patients: a randomised open-label trial. Crit Care 2009;13:R75 [MEDLINE]
MIDEX and PRODEX Trials: Dexmedetomidine vs midazolam or propofol for sedation during prolonged mechanical ventilation: two randomized controlled trials. JAMA. 2012 Mar 21;307(11):1151-60 [MEDLINE]
Role of dexmedetomidine for the prevention and treatment of delirium in intensive care unit patients. Ann Pharmacother. 2013 Jun;47(6):869-76. doi: 10.1345/aph.1AR708 [MEDLINE]
DahLIA Trial: Effect of Dexmedetomidine Added to Standard Care on Ventilator-Free Time in Patients With Agitated Delirium. JAMA. 2016 Mar 15. doi: 10.1001/jama.2016.2707 [MEDLINE]
Olanzapine vs haloperidol: treating delirium in a critical care setting. Intensive Care Med. 2004;30:444-449 [MEDLINE]
Haloperidol prophylaxis for elderly hip-surgery patients at risk for delirium: a randomized placebo-controlled study. J Am Geriatr Soc 2005;53:1658-66 [MEDLINE]
Dexmedetomidine vs. haloperidol in delirious, agitated, intubated patients: a randomised open-label trial. Crit Care 2009;13:R75 [MEDLINE]
Effect of rivastigmine as an adjunct to usual care with haloperidol on duration of delirium and mortality in critically ill patients: a multicentre, double-blind, placebo-controlled randomised trial. Lancet. 2010 Nov 27;376(9755):1829-37. doi: 10.1016/S0140-6736(10)61855-7. Epub 2010 Nov 4 [MEDLINE]
Haloperidol prophylaxis decreases delirium incidence in elderly patients after noncardiac surgery: a randomized controlled trial. Crit Care Med 2012;40:731-9 [MEDLINE]
Antipsychotic Medication for Prevention and Treatment of Delirium in Hospitalized Adults: A Systematic Review and Meta-Analysis. J Am Geriatr Soc. 2016 Apr;64(4):705-14. doi: 10.1111/jgs.14076 [MEDLINE]
Effect of Haloperidol on Survival Among Critically Ill Adults With a High Risk of Delirium: The REDUCE Randomized Clinical Trial. JAMA. 2018 Feb 20;319(7):680-690. doi: 10.1001/jama.2018.0160 [MEDLINE]
MIND-USA Trial. Haloperidol and Ziprasidone for Treatment of Delirium in Critical Illness. N Engl J Med. 2018 Dec 27;379(26):2506-2516. doi: 10.1056/NEJMoa1808217 [MEDLINE]
Antipsychotics for Preventing Delirium in Hospitalized Adults: A Systematic Review. Ann Intern Med. 2019 Sep 3. doi: 10.7326/M19-1859 [MEDLINE]
Antipsychotics for Treating Delirium in Hospitalized Adults: A Systematic Review. Ann Intern Med. 2019 Sep 3. doi: 10.7326/M19-1860 [MEDLINE]
AID-ICU Trial. Haloperidol for the Treatment of Delirium in ICU Patients. N Engl J Med. 2022 Oct 26. doi: 10.1056/NEJMoa2211868 [MEDLINE]
MENDS Trial. Effect of sedation with dexmedetomidine vs lorazepam on acute brain dysfunction in mechanically ventilated patients: the MENDS randomized controlled trial. JAMA 2007;298:2644-53 [MEDLINE]
Dexmedetomidine vs midazolam for sedation of critically ill patients: a randomized trial. JAMA 2009;301:489-9 [MEDLINE]
MIDEX and PRODEX Trials: Dexmedetomidine vs midazolam or propofol for sedation during prolonged mechanical ventilation: two randomized controlled trials. JAMA. 2012 Mar 21;307(11):1151-60 [MEDLINE]
Antipsychotic Medication for Prevention and Treatment of Delirium in Hospitalized Adults: A Systematic Review and Meta-Analysis. J Am Geriatr Soc. 2016 Apr;64(4):705-14. doi: 10.1111/jgs.14076 [MEDLINE]
Antipsychotics for Preventing Delirium in Hospitalized Adults: A Systematic Review. Ann Intern Med. 2019 Sep 3. doi: 10.7326/M19-1859 [MEDLINE]
Antipsychotics for Treating Delirium in Hospitalized Adults: A Systematic Review. Ann Intern Med. 2019 Sep 3. doi: 10.7326/M19-1860 [MEDLINE]
MIDEX and PRODEX Trials: Dexmedetomidine vs midazolam or propofol for sedation during prolonged mechanical ventilation: two randomized controlled trials. JAMA. 2012 Mar 21;307(11):1151-60 [MEDLINE]
Antipsychotic Medication for Prevention and Treatment of Delirium in Hospitalized Adults: A Systematic Review and Meta-Analysis. J Am Geriatr Soc. 2016 Apr;64(4):705-14. doi: 10.1111/jgs.14076 [MEDLINE]
Antipsychotics for Preventing Delirium in Hospitalized Adults: A Systematic Review. Ann Intern Med. 2019 Sep 3. doi: 10.7326/M19-1859 [MEDLINE]
Antipsychotics for Treating Delirium in Hospitalized Adults: A Systematic Review. Ann Intern Med. 2019 Sep 3. doi: 10.7326/M19-1860 [MEDLINE]
Rivastigmine for the prevention of postoperative delirium in elderly patients undergoing elective cardiac surgery—a randomized controlled trial. Crit Care Med. 2009;37:1762–1768 [MEDLINE]
Effect of rivastigmine as an adjunct to usual care with haloperidol on duration of delirium and mortality in critically ill patients: a multicentre, double-blind, placebo-controlled randomised trial. Lancet. 2010 Nov 27;376(9755):1829-37. doi: 10.1016/S0140-6736(10)61855-7. Epub 2010 Nov 4 [MEDLINE]
Valproic Acid for Treatment of Hyperactive or Mixed Delirium: Rationale and Literature Review. Psychosomatics. 2015 Nov-Dec;56(6):615-25. doi: 10.1016/j.psym.2015.09.008. Epub 2015 Oct 3 [MEDLINE]
Adjunctive Valproic Acid in Management-Refractory Hyperactive Delirium: A Case Series and Rationale. J Neuropsychiatry Clin Neurosci. 2015 Fall;27(4):365-70. doi: 10.1176/appi.neuropsych.14080190. Epub 2015 Mar 24 [MEDLINE]
Antipsychotic Medication for Prevention and Treatment of Delirium in Hospitalized Adults: A Systematic Review and Meta-Analysis. J Am Geriatr Soc. 2016 Apr;64(4):705-14. doi: 10.1111/jgs.14076 [MEDLINE]
MIND-USA Trial. Haloperidol and Ziprasidone for Treatment of Delirium in Critical Illness. N Engl J Med. 2018 Dec 27;379(26):2506-2516. doi: 10.1056/NEJMoa1808217 [MEDLINE]
Antipsychotics for Preventing Delirium in Hospitalized Adults: A Systematic Review. Ann Intern Med. 2019 Sep 3. doi: 10.7326/M19-1859 [MEDLINE]
Antipsychotics for Treating Delirium in Hospitalized Adults: A Systematic Review. Ann Intern Med. 2019 Sep 3. doi: 10.7326/M19-1860 [MEDLINE]
Nonpharmacologic Therapies
Positive Stimulation for Medically Sedated Patients: A Music Therapy Intervention to Treat Sedation-Related Delirium in Critical Care. Chest. 2022 Aug;162(2):367-374. doi: 10.1016/j.chest.2022.02.011 [MEDLINE]
Prognosis
Outcome of delirium in critically ill patients: systematic review and meta-analysis. BMJ. 2015 Jun 3;350:h2538. doi: 10.1136/bmj.h2538 [MEDLINE]
Association of Incident Delirium With Short-term Mortality in Adults With Critical Illness Receiving Mechanical Ventilation. JAMA Netw Open. 2022 Oct 3;5(10):e2235339. doi: 10.1001/jamanetworkopen.2022.35339 [MEDLINE]