Rhinosinusitis is Defined as the Symptomatic Inflammation of Nasal Cavity and Paranasal Sinuses
Inflammation of the Sinuses Rarely Occurs without Concomitant Nasal Mucosal Inflammation
Therefore, the Term “Rhinosinusitis” is Preferred Over “Sinusitis”
Clinical Definitions Based on Duration of Disease (Otolaryngol Head Neck Surg, 2015) [MEDLINE]
Acute Rhinosinusitis is Defined as the Presence of Symptoms for <4 wks
Subacute Rhinosinusitis is Defined as the Presence of Symptoms for 4-12 wks
Chronic Rhinosinusitis is Defined as the Presence of Symptoms for >12 wks (see Chronic Rhinosinusitis)
Recurrent Acute Rhinosinusitis is Defined as the ≥4 Episodes of Acute Rhinosinusitis Per Year (with Intervening Symptom Resolution)
Clinical Definitions Based on Etiology and Clinical Manifestations (BMJ, 2014) [MEDLINE] (Otolaryngol Head Neck Surg, 2015) [MEDLINE]
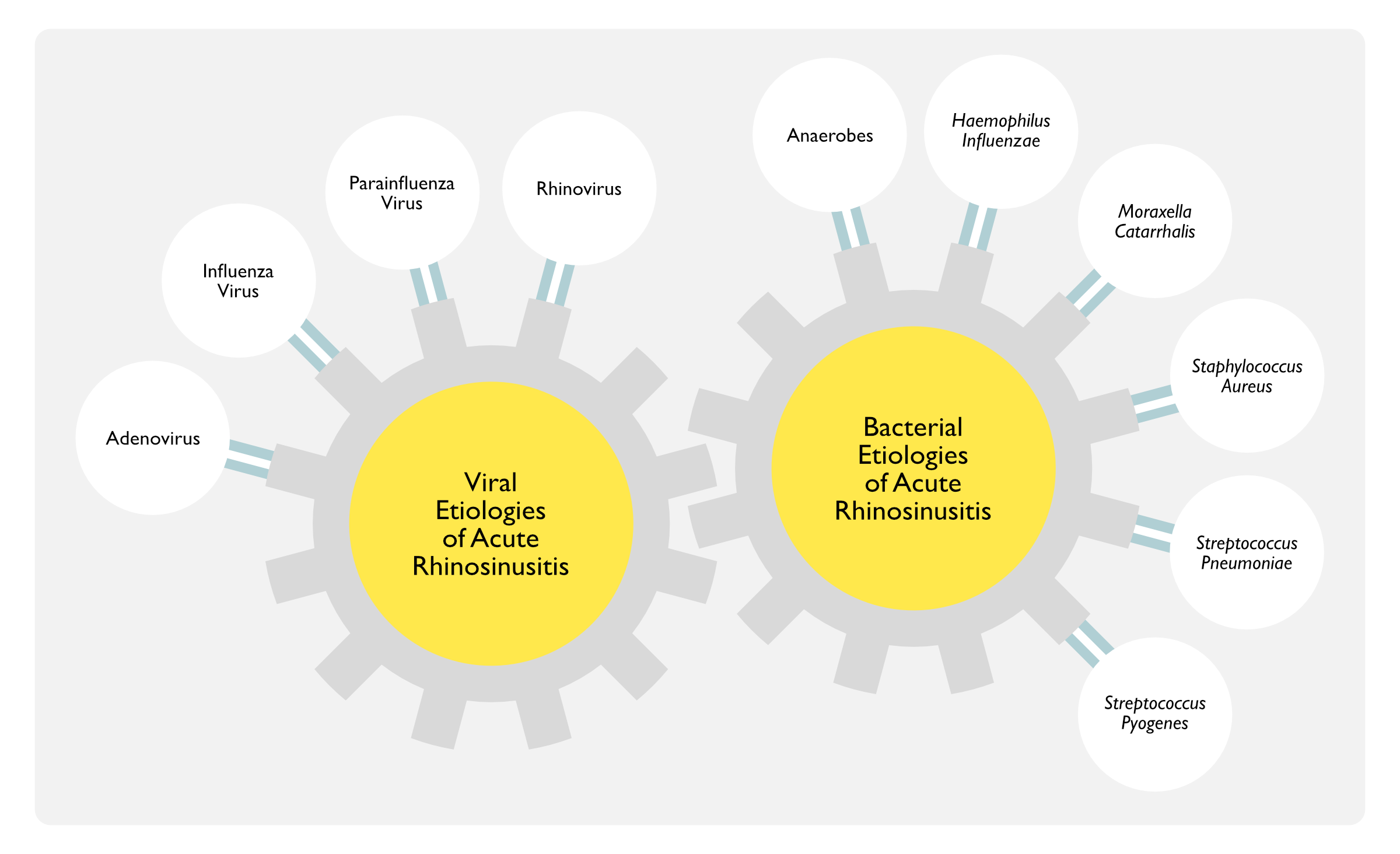
Acute Viral Rhinosinusitis
Acute Viral Rhinosinusitis is Defined as Acute Rhinosinusitis with a Viral Etiology
Uncomplicated Acute Bacterial Rhinosinusitis
Uncomplicated Acute Bacterial Rhinosinusitis is Defined as Acute Rhinosinusitis with a Bacterial Etiology without Clinical Evidence of Extension Outside of the Nasal Cavity and Paranasal Sinuses (Absence of Neurologic, Ophthalmologic, or Soft Tissue Involvement)
Presence of Purulent Nasal Drainage for Duration of <4 wks and Severe Nasal Obstruction and/or Facial Pain/Pressure/Fullness
Complicated Acute Bacterial Rhinosinusitis
Complicated Acute Bacterial Rhinosinusitis is Defined as Acute Rhinosinusitis with Bacterial Etiology with Clinical Evidence of Extension Outside of the Nasal Cavity and Paranasal Sinuses (Presence of Neurologic, Ophthalmologic, and/or Soft Tissue Involvement)
Epidemiology
Incidence
Annual Incidence of Acute Rhinosinusitis is Approximately 1 Case Per 8 Adults in the United States (12% of the Population) and Other Western Countries (Vital Health Stat, 2014) [MEDLINE] (Otolaryngol Head Neck Surg, 2015) [MEDLINE]
Approximately 30 Million Cases Per Year in the United States
Accounts for Annual Direct Health Care Costs of $11 Billion
Additional Costs Include Lost Work Productivity and Impaired Quality of Life
More than 1 in 5 Antibiotic Prescriptions in Adults are for Sinusitis (Making it the 5th Most Common Diagnosis Responsible for Antibiotic Prescription)
Age: in adults, highest incidence occurs in the 45-64 y/o group
Despite the Prevalence of Staphylococcal Colonization in the Middle Meatus in Healthy Adults, Staphylococcus Aureus Acute Bacterial Rhinosinusitis Represents Only 10% of Cases (Clin Infect Dis, 2012) [MEDLINE]
In Any Patient Presenting with an Acute Respiratory Illness, an Oropharyngeal Swab with Reverse-Transcriptase Polymerase Chain Reaction (RT-PCR) Testing for SARS-CoV-2 is Required for the Purpose of Infection Control
Anterior Rhinoscopy (Using Otoscope or Nasal Speculum) (see Rhinoscopy)
May Demonstrate Mucosal Edema, Narrowing of Middle Meatus, Hypertrophy of the Inferior Turbinate, Rhinorrhea, and/or Purulent Nasal Discharge
Nasal Polyps or Septal Deviation May Be Incidentally Detected (These Findings are Preexisting Anatomic Risk Factors for the Development of Acute Bacterial Rhinosinusitis)
Recommended in Patients with Ear Fullness/Pressure/Otalgia to Diagnose Otitis Media, etc
Transillumination of Sinuses (CMAJ, 1997) [MEDLINE]
Transillumination of Sinuses is Not Recommended
Limited to Examination of Frontal and Maxillary Sinuses
Low Sensitivity and Low Specificity
Culture of Nasal Discharge or Nasal Swabs
Nasal/Oropharyngeal Viral and Bacterial Cultures are Not Recommended
Culture of Secretions from the Nasal Cavity or Nasopharynx Does Not Differentiate Acute Viral Rhinosinusitis from Acute Bacterial Rhinosinusitis, Because Nasal Cultures Correlate Poorly with Maxillary Sinus Cultures Obtained by Direct Aspiration (Otolaryngol Head Neck Surg, 2015) [MEDLINE]
Recommendations for Failure to Respond to Both First/Second-Line Antibiotics (i.e. Second Course of Antibiotics) (Infectious Diseases Society of America-IDSA Clinical Practice Guideline for Acute Bacterial Rhinosinusitis in Children and Adults) (Clinical Infectious Diseases, 2012) [MEDLINE]
In Patients with Acute Bacterial Rhinosinusitis Who Have Failed to Respond to Both First/Second-Line Antibiotics, It is Recommended that Cultures Be Obtained by Direct Sinus Aspiration Rather than By Nasopharyngeal Swab in Patients with Suspected Sinus Infection Who Have Failed to Respond to Empiric Antibiotics (Strong Recommendation, Moderate Quality of Evidence)
Nasopharyngeal Cultures are Unreliable and are Not Recommended for the Microbiologic Diagnosis of Acute Bacterial Rhinosinusitis (Strong Recommendation, High Quality of Evidence)
In Adults with Acute Bacterial Rhinosinusitis Who Have Failed to Respond to Both First/Second-Line Antibiotics, Endoscopically-Guided Cultures of the Middle Meatus May Be Considered (But Their Reliability in Children Has Not Been Established) (Weak Recommendation, Moderate Quality of Evidence)
Antral/Maxillary Sinus Puncture (Otolaryngol Head Neck Surg, 2002) [MEDLINE]
Not Usually Necessary
Recommendations for Failure to Respond to Both First/Second-Line Antibiotics (i.e. Second Course of Antibiotics) (Infectious Diseases Society of America-IDSA Clinical Practice Guideline for Acute Bacterial Rhinosinusitis in Children and Adults) (Clinical Infectious Diseases, 2012) [MEDLINE]
In Patients with Acute Bacterial Rhinosinusitis Who Have Failed to Respond to Both First/Second-Line Antibiotics, It is Recommended that Cultures Be Obtained by Direct Sinus Aspiration Rather than By Nasopharyngeal Swab in Patients with Suspected Sinus Infection Who Have Failed to Respond to Empiric Antibiotics (Strong Recommendation, Moderate Quality of Evidence)
Nasopharyngeal Cultures are Unreliable and are Not Recommended for the Microbiologic Diagnosis of Acute Bacterial Rhinosinusitis (Strong Recommendation, High Quality of Evidence)
In Adults with Acute Bacterial Rhinosinusitis Who Have Failed to Respond to Both First/Second-Line Antibiotics, Endoscopically-Guided Cultures of the Middle Meatus May Be Considered (But Their Reliability in Children Has Not Been Established) (Weak Recommendation, Moderate Quality of Evidence)
Recommendations for Failure to Respond to Both First/Second-Line Antibiotics (i.e. Second Course of Antibiotics) (Infectious Diseases Society of America-IDSA Clinical Practice Guideline for Acute Bacterial Rhinosinusitis in Children and Adults) (Clinical Infectious Diseases, 2012) [MEDLINE]
In Patients with Acute Bacterial Rhinosinusitis Who Have Failed to Respond to Both First/Second-Line Antibiotics, It is Recommended that Cultures Be Obtained by Direct Sinus Aspiration Rather than By Nasopharyngeal Swab in Patients with Suspected Sinus Infection Who Have Failed to Respond to Empiric Antibiotics (Strong Recommendation, Moderate Quality of Evidence)
Nasopharyngeal Cultures are Unreliable and are Not Recommended for the Microbiologic Diagnosis of Acute Bacterial Rhinosinusitis (Strong Recommendation, High Quality of Evidence)
In Adults with Acute Bacterial Rhinosinusitis Who Have Failed to Respond to Both First/Second-Line Antibiotics, Endoscopically-Guided Cultures of the Middle Meatus May Be Considered (But Their Reliability in Children Has Not Been Established) (Weak Recommendation, Moderate Quality of Evidence)
Sinus Imaging
General Comments
Sinus Imaging is Not indicated in the Initial Evaluation of Uncomplicated Acute Rhinosinusitis
Indications for Sinus Imaging
Recurrent/Treatment-Resistant Rhinosinusitis (Non-Contrast Sinus CT is Sufficient for This Purpose)
To Diagnose Blockage of the Ostio-Meatal Complex
Suspicion of Orbital/Intracranial Extension (Contrast Sinus CT is Required for This Purpose)
Recommendations (Infectious Diseases Society of America-IDSA Clinical Practice Guideline for Acute Bacterial Rhinosinusitis in Children and Adults) (Clinical Infectious Diseases, 2012) [MEDLINE]
In Patients with Acute Bacterial RHinosinusitis Suspected to Have Suppurative Complications, Axial and Coronal Views of Contrast-Enhanced Sinus CT (Rather than Magnetic Resonance Imaging) is Recommended to Localize the Infection and Guide Further Treatment (Weak Recommendation, Low Quality of Evidence)
Recommendations (American Academy of Otolaryngology-Head and Neck Surgery Clinical Practice Guideline for Adult Sinusitis) (Otolaryngol Head Neck Surg, 2015) [MEDLINE]
Clinicians Should Not Obtain Radiographic Imaging in Acute Rhinosinusitis, Unless a Complication or Alternative Diagnosis is Suspected (Recommendation Against Imaging if Based on Diagnostic Studies with Minor Limitations and a Preponderance of Benefit Over Harm for Not Obtaining Imaging
When Imaging is Indicated (by Indication Above), Sinus Computed Tomography is the Procedure of Choice (Clin Infect Dis, 2012) [MEDLINE] (Otolaryngol Head Neck Surg, 2015) [MEDLINE]
Typical Radiographic Findings in Acute Rhinosinusitis
Sinus Air-Fluid Levels (with AIr Bubbles within the Sinuses)
In Patient with Common Cold, 87% of Cases Manifested Sinus Air-Fluid Levels and/or Mucosal Thickening When Assessed within 2-3 days of Symptom Onset (NEJM, 1994) [MEDLINE]
Sinus Mucosal Edema
However, Some Form of Sinus Mucosal Abnormality Can Be Identified on Sinus CT in 42% of Asymptomatic Healthy Persons (Arch Otolaryngol Head Neck Surg, 1988) [MEDLINE] (Laryngoscope, 1991) [MEDLINE]
In Patient with Common Cold, 87% of Cases Manifested Sinus Air-Fluid Levels and/or Mucosal Thickening When Assessed within 2-3 days of Symptom Onset (NEJM, 1994) [MEDLINE]
While the Initial Clinical Presentation Has Limited Accuracy in Differentiating Acute Viral Rhinosinusitis from Acute Bacterial Rhinosinusitis, These Disorders Have Different Clinical Courses (Lancet, 2008) [MEDLINE] (Clin Infect Dis, 2012) [MEDLINE]
Clinical Features of Both Acute Viral Rhinosinusitis and Acute Bacterial Rhinosinusitis
Fever is Present in Some Acute Viral Rhinosinusitis Cases in the First Few Days of Illness, But it Does Not Predict Presence of Acute Bacterial Rhinosinusitis (Otolaryngol Head Neck Surg, 2015) [MEDLINE]
Fever Has a Sensitivity of Only 50% for Acute Bacterial Rhinosinusitis (Otolaryngol Head Neck Surg, 2015)* [MEDLINE]
Fever May Be the Only Sign of Acute Bacterial Rhinosinusitis in Hospital-Acquired Cases
Symptoms of the Common Cold and Acute Rhinosinusitis Often Overlap (see Common Cold)
However, Facial Pain is Typically Absent in the Common Cold
Clinical Course
Similar to Other Viral Upper Respiratory Infections, Acute Viral Rhinosinusitis Manifests Partial/Complete Resolution within 7-10 Days (ORL J Otorhinolaryngol Relat Spec, 1976) [MEDLINE] (Ann Otol Rhinol Laryngol, 1983) [MEDLINE] (Acta Otolaryngol, 1988) [MEDLINE] (Ann Intern Med, 1992) [MEDLINE] (Allergy, 2005) [MEDLINE] (Otolaryngol Head Neck Surg, 2015) [MEDLINE]
Symptoms Typically Peak Between Days 3-6 and Then, Subsequently Improve
In Patients in Which Clinical Symptoms Persist for >10 Days, There is Generally Some Clinical Improvement by Day 10 (JAMA, 1967) [MEDLINE]
Most Commonly, the Nasal Discharge Starts Clear, Then Turns Purulent (Due to Nasal/Sinus Mucosal Inflammation), and Subsequently, Turns Clear Again
If Fever Occurs, it Generally is Present Early in the Illness and Resolves withint the First 24-48 hrs (Clin Infect Dis, 2012) [MEDLINE]
Respiratory Symptoms Become More Prominent as the Fever Resolves
Transition from Viral to Bacterial Infection
Acute Viral Rhinosinusitis is Complicated by Bacterial Rhinosinusitis in Only 0.5-2% of Cases (Rhinol Suppl, 2012) [MEDLINE]
Acute Bacterial Rhinosinusitis
Clinical Course
Purulent Nasal Discharge/Facial Pain Cannot Be Used to Distinguish Acute Viral Rhinosinusitis from Acute Bacterial Rhinosinusitis (Acta Otolaryngol, 1988) [MEDLINE] (Otolaryngol Head Neck Surg, 2014) [MEDLINE] (Otolaryngol Head Neck Surg, 2014) [MEDLINE]
Clinical Features (Any of the Following) Suggest the Diagnosis of Acute Bacterial Rhinosinusitis Over Acute Viral Rhinosinusitis (Infectious Diseases Society of America (IDSA) Clinical Practice Guideline for Acute Bacterial Rhinosinusitis in Children and Adults; Criteria Have Not Been Rigorously Evaluated) (Clin Infect Dis, 2012) [MEDLINE] (Otolaryngol Head Neck Surg, 2015) [MEDLINE]
Persistent Symptoms/Signs of Acute Rhinosinusitis (Nasal Discharge/Fever/Headache/Facial Pain) Lasting for ≥10 Days without Any Evidence of Clinical Improvement (Strong Recommendation, Low-Moderate Quality Evidence)
Although Viral Symptoms May Persist for >10 Days in Some Cases, There is Generally Some Clinical Improvement by Day 10
However, in Trials, Only 60% of Adults with Symptoms for >7-10 Days Had a Bacterial Etiology Identified by Sinus Aspirate
Onset of Severe Symptoms or High Fever (≥39°C/102°F) and Purulent Nasal Discharge/Facial Pain Lasting at Least 3-4 Consecutive Days at the Beginning of the Illness (Strong Recommendation, Low-Moderate Quality Evidence)
Fever Associated with Viral Rhinosinusitis Usually Subsides in 24-48 hrs
Purulent Nasal Discharge Associated with Viral Rhinosinusitis Usually Occurs 4-5 Days into the Illness
Biphasic “Double-Worsening” Pattern (New Onset of Fever, Worsening of Fever/Headache or Increased Nasal Discharge) Following a Typical Acute Viral Rhinosinusitis Which Lasted 5-6 Days and Were Initially Improving (Strong Recommendation, Low-Moderate Quality Evidence) (J Allergy Clin Immunol, 1992) [MEDLINE] (Fam Med, 1996) [MEDLINE] (Br J Gen Pract, 2002) [MEDLINE]
Symptoms/Signs on an Acute Rhinosinusitis (New Onset of Fever/Headache/Nasal Discharge) Which Initially Start to Improve, Then Worsen Approximately 5-6 Days Later
Recommendations (American Academy of Otolaryngology-Head and Neck Surgery Clinical Practice Guideline for Adult Sinusitis) (Otolaryngol Head Neck Surg, 2015) [MEDLINE]
Clinicians Should Distinguish Acute Bacterial Rhinosinusitis from Acute Viral Rhinosinusitis (and Rhinosinusitis Caused by Noninfectious Conditions) (Strong Recommendation Based on Diagnostic Studies with Minor Limitations and a Preponderance of Benefit Over Harm)
Clinician Should Diagnose Acute Bacterial Rhinosinusitis When Either of the Following is Present (Strong Recommendation Based on Diagnostic Studies with Minor Limitations and a Preponderance of Benefit Over Harm)
Symptoms/Signs of Acute Rhinosinusitis (Purulent Nasal Drainage with Nasal Obstruction and/or Facial Pain/Pressure/Fullness) Persist without Clinical Improvement for a Duration of at Least 10 Days (Starting from Onset of Respiratory Symptoms)
However, Guidelines Acknowledge that There is No High-Level Evidence Demonstrating that Symptom Duration and Purulent Discharge Can Reliably Distinguish Between Acute Bacterial Rhinosinusitis and Acute Viral Rhinosinusitis
Symptoms/Signs of Acute Rhinosinusitis Worsen within 10 Days After Initial Clinical Improvement (“Double Worsening” Pattern)
Clinicians Should Differentiate Chronic Rhinosinusitis and Recurrent Acute Rhinosinusitis from Isolated Episodes of Acute Bacterial Rhinosinusitis and Other Causes of Sinonasal Symptoms (Recommendation Based on Cohort and Observational Studies with a Preponderance of Benefit Over Harm)
Clinicians Should Assess the Patient with Chronic Rhinosinusitis or Recurrent Acute Rhinosinusitis for Chronic Conditions Which Would Modify Management (Recommendation Based on One Systematic Review and Multiple Observational Studies with a Preponderance of Benefit Over Harm)
Ciliary Dyskinesia is Associated with Chronic Rhinosinusitis (see Chronic Rhinosinusitis)
Clinician May Obtain Testing for Allergy and Immune Function in Evaluating a Patient with Chronic Rhinosinusitis or Recurrent Acute Rhinosinusitis (Option Based on Observational Studies with an Unclear Balance of Benefit vs Harm)
Clinical Definitions of Uncomplicated vs Complicated Bacterial Rhinosinusitis (BMJ, 2014) [MEDLINE] (Otolaryngol Head Neck Surg, 2015) [MEDLINE]
Uncomplicated Acute Bacterial Rhinosinusitis
Defined as Acute Rhinosinusitis with a Bacterial Etiology without Clinical Evidence of Extension Outside of the Nasal Cavity and Paranasal Sinuses (Absence of Neurologic, Ophthalmologic, or Soft Tissue Involvement)
Presence of Purulent Nasal Drainage for Duration of <4 wks and Severe Nasal Obstruction and/or Facial Pain/Pressure/Fullness
Complicated Acute Bacterial Rhinosinusitis
Defined as Acute Rhinosinusitis with Bacterial Etiology with Clinical Evidence of Extension Outside of the Nasal Cavity and Paranasal Sinuses (Presence of Neurologic, Ophthalmologic, and/or Soft Tissue Involvement)
Supportive Care is Recommended, as No Known Treatments Shorten the Duration of Acute Viral Rhinosinusitis (BMJ, 2008) [MEDLINE]
Recommendations (American Academy of Otolaryngology-Head and Neck Surgery Clinical Practice Guideline for Adult Sinusitis) (Otolaryngol Head Neck Surg, 2015) [MEDLINE]
Clinicians May Recommend Analgesics, Intranasal Corticosteroids, and/or Nasal Saline Irrigation for Symptomatic Relief of Acute Viral Rhinosinusitis (Option Based on Randomized Controlled Trials with Limitations and Cohort Studies with an Unclear Balance of Benefit and Harm Which Varies by Patient)
Limit/Avoid Use of Acetaminophen in Patients with Liver Disease
Cautious Use or Avoid Use of NSAID’s in Patients with Liver Disease, Cardiovascular Disease, or Chronic Kidney Disease
NSAID’s are Associated with Increased Risk of Gastrointestinal Upset/Hemorrhage
Recommendations
Useful for the Treatment of Fever/Pain Associated with Acute Viral Rhinosinusitis (Clin Infect Dis, 2012) [MEDLINE] (Otolaryngol Head Neck Surg, 2015) [MEDLINE]
Intranasal (Sterile) Saline Spray or Lavage
Lavage Preparations
Buffered Saline
Physiologic Saline
Hypertonic Saline
Technique
Irrigate Nasal Passages with Sterile Saline Lavage Solution 1-2x Per Day
Efficacy
May Temporarily Improve Nasal Passage Patency
Nasal Saline Irrigation is Useful to Relieve the Symptoms of Acute Upper Respiratory Tract Infection (Although Trials were Small and Had High Risk of Bias) (Cochrane Database Syst Rev, 2015) [MEDLINE]
Moisturizes Nasal Passages
Loosens Secretions
Useful in Conjunction with Intranasal Corticosteroids
May Be Particularly Useful in Patients with Recurrent Sinus Infections
Precautions
Use of Non-Sterile Saline (or Tap Water) May Introduce Infection
Case Reports of Amebic Encephalitis When Tap Water was Used for Nasal Irrigation (Int J Infect Dis, 2018) [MEDLINE]
May Cause Nasal Burning/Irritation
Some Patients are Unable to Tolerate (Particularly When Using a Neti Pot-Type Device, etc)
Recommendations
Useful for the Treatment of Symptoms Associated with Acute Viral Rhinosinusitis (Clin Infect Dis, 2012) [MEDLINE] (Cochrane Database Syst Rev, 2015) [MEDLINE] (Otolaryngol Head Neck Surg, 2015) [MEDLINE]
Mometasone (Nasonex, Asmanex, Elocon) (see Mometasone)
Triamcinolone (Kenalog, Nasacort, Adcortyl) (see Triamcinolone)
Efficacy
Intranasal Corticosteroids Decrease Inflammation, Resulting in Relief of Congestion and Promotion of Sinus Drainage
In a Systematic Review, Intranasal Corticosteroids Relieved Facial Pain and Nasal Congestion in Patients with Acute Rhinosinusitis (Ann Fam Med, 2012) [MEDLINE]
Magnitude of the Effect was Small (At 14-21 Days, 66% of Patients Improved with Placebo vs 73% of Patients Improved with Intranasal Corticosteroid Therapy)
Adverse Effects were Minimal
In a Meta-Analysis of Intranasal Corticosteroids in the Treatment of Acute Sinusitis, Intranasal Corticosteroids Increased the Rate of Symptom Response (When Used with or without Concomitant Antibiotics), as Compared to Placebo (Cochrane Database Syst Rev, 2013) [MEDLINE]
Intranasal Corticosteroids May Be Especially Useful in Patients with Preexisting Allergic Rhinitis (see Allergic Rhinitis)
Precautions
Intranasal Corticosteroids Can Cause Epistaxis and/or Sore Throat
Recommendations
Although Intranasal Corticosteroids Do Not Have an FDA Approval for This Indication, When Used Short-Term, They May Be Useful for the Treatment of Acute Viral and Bacterial Rhinosinusitis (Clin Infect Dis, 2012) [MEDLINE] (Otolaryngol Head Neck Surg, 2015) [MEDLINE]
May Improve Nasal Patency and Promote Nasal Drainage
Little Benefit as an Adjunctive Therapy to Antibiotics in Acute Bacterial Rhinosinusitis
Precautions
Avoid Use for >3 Days, as it May Cause Rebound Nasal Congestion or Mucosal Damage with Prolonged Use (J Allergy Clin Immunol, 1998) [MEDLINE]
In Animal Models, Intranasal Decongestants Have Been Demonstrated to Actually Promote Mucosal Inflammation (Ann Otol Rhinol Laryngol, 1996) [MEDLINE]
Recommendations
No Evidence for Clinical Efficacy in the Treatment Acute Viral Rhinosinusitis (Clin Infect Dis, 2012) [MEDLINE] (Otolaryngol Head Neck Surg, 2015) [MEDLINE]
Oral Decongestants
Agents
Ephedrine (Akovaz, Corphedra, Emerphed) (see Ephedrine)
Phenylephrine (Neo-Synephrine, Sudafed PE, Sudafed PE Congestion, PediaCare Children’s Decongestant, etc) (see Phenylephrine)
Phenylpropanolamine (Phenyldrine, Propan, Propagest) (see Phenylpropanolamine)
Due to Sympathomimetic Effects, Avoid or Cautious Use in Patients with Cardiovascular Disease, Hypertension, Angle-Closure Glaucoma, or Bladder Neck Obstruction (J Am Geriatr Soc, 1982) [MEDLINE]
Recommendations
When Eustachian Tube Dysfunction is Present, Oral Decongestants May Be Useful in the Treatment of Acute Viral Rhinosinusitis
In Other Patients with Acute Viral Rhinosinusitis, Their Benefit Appears to Be Outweighed by Their Adverse Effects
Mucosal Drying Effect (This Effect May Worsen Symptoms by Resulting in Thickened, Difficult to Mobilize Secretions)
Recommendations
No Evidence for Clinical Efficacy in the Treatment Acute Viral Rhinosinusitis (Clin Infect Dis, 2012) [MEDLINE] (Otolaryngol Head Neck Surg, 2015) [MEDLINE]
Oral Expectorants/Mucolytics
Agents
Guaifenesin (Robitussin, Mucinex) (see Guaifenesin)
Efficacy
May Promote Drainage by Thinning Secretions
Precautions
May Cause Gastrointestinal Upset and Drowsiness
Recommendations
No Evidence for Clinical Efficacy in the Treatment Acute Viral Rhinosinusitis (Clin Infect Dis, 2012) [MEDLINE] (Otolaryngol Head Neck Surg, 2015) [MEDLINE]
Steam Inhalation
Efficacy
Inhalation of Warm, Humidified Air (Steam) May Relieve Nasal Congestion
No Evidence that Steam Inhalation Shortens the Duration of Symptoms in Acute Viral Rhinosinusitis (Cochrane Database Syst Rev, 2013) [MEDLINE] (CMAJ, 2016) [MEDLINE]
Precautions
Avoid Contamination with Mold and Other Substances
Recommendations
Unclear Clinical Benefit
Treatment of Acute Bacterial Rhinosinusitis
General Comments
Recommendations (American Academy of Otolaryngology-Head and Neck Surgery Clinical Practice Guideline for Adult Sinusitis) (Otolaryngol Head Neck Surg, 2015) [MEDLINE]
Clinicians May Recommend Analgesics, Intranasal Corticosteroids, and/or Nasal Saline Irrigation for Symptomatic Relief of Acute Bacterial Rhinosinusitis (Option Based on Randomized Controlled Trials with Heterogeneous Populations, Diagnostic Criteria, and Outcome Measures with a Balance of Benefit and Harm)
Removal of Nasal Devices (When Present in Hospital-Acquired Acute Bacterial Rhinosinusitis)
Removal of Nasogastric Tubes/Removal of Nasal Packing/Avoidance of Nasaotracheal Intubation
Oral Analgesics
See Above
Intranasal (Sterile) Saline Spray or Lavage
See Above
Recommendations (Infectious Diseases Society of America-IDSA Clinical Practice Guideline for Acute Bacterial Rhinosinusitis in Children and Adults) (Clinical Infectious Diseases, 2012) [MEDLINE]
Intranasal Saline Irrigation with Either Physiologic or Hypertonic Saline is Recommended as an Adjunctive Treatment in Adults with Acute Bacterial Rhinosinusitis (Weak Recommendation, Low-Moderate Quality of Evidence)
Mometasone (Nasonex, Asmanex, Elocon) (see Mometasone)
Triamcinolone (Kenalog, Nasacort, Adcortyl) (see Triamcinolone)
Efficacy
Decrease Inflammation, Resulting in Relief of Congestion and Promotion of Sinus Drainage
When Used as an Adjunct to Antibiotic Therapy in the Treatment of Acute Bacterial Rhinosinusitis, a Meta-Analysis of Placebo-Controlled Trials Suggested that 15 Patients Would Need to Be Treated with Intranasal Glucocorticoids to Improve Clinical Symptoms in 1 Patient (Clin Infect Dis, 2012) [MEDLINE]
In a Meta-Analysis of Intranasal Corticosteroids in the Treatment of Acute Sinusitis, Intranasal Corticosteroids Increased the Rate of Symptom Response (When Used with or without Concomitant Antibiotics), as Compared to Placebo (Cochrane Database Syst Rev, 2013) [MEDLINE]
May Be Especially Useful in Patients with Preexisting Allergic Rhinitis (see Allergic Rhinitis)
Precautions
Intranasal Corticosteroids Can Cause Epistaxis and/or Sore Throat
Recommendations (Infectious Diseases Society of America-IDSA Clinical Practice Guideline for Acute Bacterial Rhinosinusitis in Children and Adults) (Clinical Infectious Diseases, 2012) [MEDLINE]
Intranasal Corticosteroids are Recommended as an Adjunct to Antibiotics in the Treatment of Acute Bacterial Rhinosinusitis, Primarily in Patients with a History of Allergic Rhinitis (Weak Recommendation, Moderate Quality of Evidence)
Recommendations (American Academy of Otolaryngology-Head and Neck Surgery Clinical Practice Guideline for Adult Sinusitis) (Otolaryngol Head Neck Surg, 2015) [MEDLINE]
Although Intranasal Corticosteroids Do Not Have an FDA Approval for This Indication, When Used Short-Term, They May Be Useful for the Treatment of Acute Viral and Bacterial Rhinosinusitis
Systemic Review/Meta-Analysis of Systemic Corticosteroids for Acute Rhinosinusitis (Cochrane Database Syst Rev, 2011) [MEDLINE]: n = 4 randomized trials
Systemic Corticosteroids with Antibiotics Improved Symptom Control at Days 3-7, as Compared to Antibiotics with Placebo (or in One Trial, a Nonsteroidal Anti-Inflammatory Drug)
Randomized Trial of Systemic Corticosteroid Monotherapy for Clinically Diagnosed Acute Rhinosinusitis (CMAJ, 2012) [MEDLINE]
Systemic Corticosteroids Had No Clinical Benefit
Systematic Review of Systemic Corticosteroid Monotherapy in Acute Bacterial Rhinosinusitis (Cochrane Database Syst Rev, 2014) [MEDLINE]
Overall, Systemic Corticosteroids Had No Clinical Benefit
Limited Data from 5 Trials Suggested that Systemic Corticosteroids Used in Combination with Antibiotics May Have a Modest Short-Term Beneficial Effect on Symptom Relief (Number Needed to Treat of 7), But Confidence in the Results was Limited
Recommendations
Systemic Corticosteroids are Not Recommended Until Further High-Quality Trials are Performed
Intranasal Ipratropium Bromide
See Above
Intranasal Decongestants
See Above
Recommendations (Infectious Diseases Society of America-IDSA Clinical Practice Guideline for Acute Bacterial Rhinosinusitis in Children and Adults) (Clinical Infectious Diseases, 2012) [MEDLINE]
Neither Topical Nor Oral Decongestants and/or Antihistamines are Recommended as Adjunctive Treatment in Patients with Acute Bacterial Rhinosinusitis (Strong Recommendation, Low-Moderate Quality of Evidence)
Oral Decongestants
See Above
Recommendations (Infectious Diseases Society of America-IDSA Clinical Practice Guideline for Acute Bacterial Rhinosinusitis in Children and Adults) (Clinical Infectious Diseases, 2012) [MEDLINE]
Neither Topical Nor Oral Decongestants and/or Antihistamines are Recommended as Adjunctive Treatment in Patients with Acute Bacterial Rhinosinusitis (Strong Recommendation, Low-Moderate Quality of Evidence)
Oral Antihistamines
Recommendations (Infectious Diseases Society of America-IDSA Clinical Practice Guideline for Acute Bacterial Rhinosinusitis in Children and Adults) (Clinical Infectious Diseases, 2012) [MEDLINE]
Neither Topical Nor Oral Decongestants and/or Antihistamines are Recommended as Adjunctive Treatment in Patients with Acute Bacterial Rhinosinusitis (Strong Recommendation, Low-Moderate Quality of Evidence)
Recommendations (American Academy of Otolaryngology-Head and Neck Surgery Clinical Practice Guideline for Adult Sinusitis) (Otolaryngol Head Neck Surg, 2015) [MEDLINE]
Useful in Acute Bacterial Rhinosinusitis Only in Atopic Patients (Otolaryngol Head Neck Surg, 2015) [MEDLINE]
Guaifenesin Has No Proven Clinical Efficacy in the Treatment of Acute Bacterial Rhinosinusitis (Otolaryngol Head Neck Surg, 2015) [MEDLINE]
Steam Inhalation
See Above
Antibiotics
Use of Antibiotics in Acute Bacterial Rhinosinusitis
Due to the Difficulty Distinguishing Acute Viral Rhinosinusitis from Acute Bacterial Rhinosinusitis, Inappropriate Antibiotic Use Has Historically Been Common
In the US, 85-98% of Patients Receive Antibiotics for Upper Respiratory or Sinus Infection (Despite the Vast Majority of These Representing Viral Rhinosinusitis, for Which Antibiotics are Ineffective) (Ann Intern Med, 2001) [MEDLINE]
Clinical Efficacy of Antibiotics in Acute Rhinosinusitis
Systematic Review of 10 Trials of Antibiotics in Patients with Uncomplicated Acute Sinusitis and Normal Immune System (Cochrane Database Syst Rev, 2012) [MEDLINE]
Antibiotics Slightly Shortened the Time to Cure, But Increased the Rate of Adverse Effects
Systematic Review of 5 Trials of Antibiotics in Acute Maxillary Sinusitis (Cochrane Database Syst Rev, 2014)
Antibiotics Provided a Small Clinical Benefit in Immunocompetent Primary Care Patients with Uncomplicated Acute Sinusitis (Risk of Clinical Failure Had Pooled Risk Ratio of 0.66; 95% CI: 0.47-0.94)
However, About 86% of Patients Treated Without Antibiotics Improved Within 2 wks
Summary of Systematic Reviews (Otolaryngol Head Neck Surg, 2015) [MEDLINE]
Cure or Improvement Rates at 7-15 Days Favored Antibiotic, But the Clinical Benefit was Small (91% for Antibiotic Therapy vs 86% for Placebo)
Number Needed to Treat for Benefit Ranged from 11-15 Patients and Odds Ratios for Overall Treatment Effect Ranged from 1.25-1.87
Duration of Pain/Illness Associated with Acute Bacterial Rhinosinusitis Did Not Demonstrate Any Consistent Relationship to Initial Management
Adverse Events were More Common in the Antibiotic-Treated Patients (Odds Ratios: 1.87-2.10; Number Needed to Harm: 8.1), But the Rate of Dropout Due to Adverse Events was Small (1%-1.5%) and Similar Between Both Groups
Complications were Similar Regardless of Initial Management
Systematic Review of Antibiotics in Uncomplicated Acute Rhinosinusitis in Immunocompetent Patients in Ambulatory Care Settings (Cochrane Database Syst Rev, 2018) [MEDLINE]: n= 3,000 (15 randomized trials)
Trial Included Patients with Acute Rhinosinusitis-Like Symptoms/Signs or Sinusitis Confirmed by Imaging
Approximately 66% of Patients Improved by 2 wk, Irrespective of Antibiotic Therapy
However, Since Trials May Have Included Some Patients with Acute Viral Rhinosinusitis, Rates of Recovery from Populations of Patients with Pure Acute Bacterial Rhinosinusitis May Be Lower Thna Reported in These Studies
Antibiotic-Treated Patients Had Increased Risk of Adverse Events
Authors Conclusions
Potential Benefit of Antibiotics to Treat Acute Rhinosinusitis Diagnosed Either Clinically (Low Risk of Bias, High-Quality Evidence) or Confirmed by Imaging (Low-Unclear Risk of Bias, Moderate-Quality Evidence) is Marginal
They Concluded that There is No Role for Antibiotics in the Treatment of Acute Rhinosinusitis
They Could Not Draw Conclusions About a Role for Antibiotics in the Treatment of Acute Rhinosinusitis in Children/Immunocompromised/Those with Severe Sinusiti (as These Populations were Not Included in the Available Trials)
Recommendations (Infectious Diseases Society of America-IDSA Clinical Practice Guideline for Acute Bacterial Rhinosinusitis in Children and Adults) (Clinical Infectious Diseases, 2012) [MEDLINE]
Empiric Antibiotics Should Be Initiated as Soon as the Clinical Diagnosis of Acute Bacterial Rhinosinusitis is Established as Defined Above (Strong Recommendation, Moderate Quality of Evidence)
Recommendations (American Academy of Otolaryngology-Head and Neck Surgery Clinical Practice Guideline for Adult Sinusitis) (Otolaryngol Head Neck Surg, 2015) [MEDLINE]
Clinicians Should Either Offer Watchful Waiting (Without Antibiotics) or Prescribe Initial Antibiotic Therapy for Adults with Uncomplicated Acute Bacterial Rhinosinusitis (Recommendation Based on Systematic Reviews of Double-Blind Randomized Controlled Trials with Some Heterogeneity in Diagnostic Criteria and Illness Severity and a Relative Balance of Benefit and Risk)
Watchful Waiting Should Be Offered Only When There is Reliable Follow-Up
Antibiotic Therapy Should Be Started if the Patient’s Condition Fails to Improve by 7 Days After Acute Bacterial Rhinosinusitis Diagnosis or if it Worsens at Any Time
Patient Can Be Given a Wait-and-See Antibiotic Prescription (WASP) or a Safety Ney Antibiotic Prescription (SNAP) to Avoid a Second Office Visit, If Antibiotics are to Required
If the Patient Fails to Improve with the Initial Management Option by 7 Days After Diagnosis or Worsens During the Initial Management, Clinician Should Reassess the Patient to Confirm the Diagnosis of Acute Bacterial Rhinosinusitis, Exclude Other Etiologies, and Detect Complications (Recommendation Based on Randomized Controlled Trials with Limitations Supporting a Cut-Point of 7 Days for Lack of Improvement and Expert Opinion and First Principles for Changing Therapy with a Preponderance of Benefit Over Harm)
If Acute Bacterial Rhinosinusitis is Diagnosed in the Patient Initially Managed with Observation, Clinician Should Begin Antibiotics
If the Patient was Initially Managed with Antibiotics, Clinician Should Change the Antibiotic
Recommendations-General
Since Immunocompromised Patients were Not Included in Trials (and Patients with Immune-Modifying Comorbid Conditions, such as Diabetes Mellitus, etc May Have Altered Immune Response), Antibiotic Treatment of Acute Bacterial Rhinosinusitis Should Be Individualized and Early Treatment May Be Warranted (NEJM, 2016) [MEDLINE]
Choice of Antibiotic Agent
Recommendations (American Academy of Otolaryngology-Head and Neck Surgery Clinical Practice Guideline for Adult Sinusitis) (Otolaryngol Head Neck Surg, 2015) [MEDLINE]
If a Decision is Made to Treat Acute Bacterial Rhinosinusitis with Antibiotics, Amoxicillin with or without Clavulanic Acid Should Be First-LIne Therapy (For 5-10 Days) for Most Adults (Recommendation Based on Randomized Controlled Trials with Heterogeneity and Noninferiority Design with a Preponderance of Benefit Over Harm)
Factors Favoring the Use of Amoxicillin-Clavulanic Acid Over Amoxicillin
Factors Increasing the Risk of Bacterial Resistance
Antibiotic Use in the Past Month
Breakthrough Infection Despite Prophylaxis
Close Contact with a Child in a Daycare Facility
Close Contact with Treated Individuals, Health Care Providers, or a Health Care Environment
Failure of Prior Antibiotic Therapy
High Prevalence of Resistant Bacteria in Community
Smoker (or Smoker in the Family)
Factors Indicating Moderate-Severe Infection
Frontal/Sphenoidal Sinusitis
History of Recurrent Acute Bacterial Rhinosinusitis
Recommendations (Infectious Diseases Society of America-IDSA Clinical Practice Guideline for Acute Bacterial Rhinosinusitis in Children and Adults) (Clinical Infectious Diseases, 2012) [MEDLINE]
Amoxicillin-Clavulanic Acid (Rather than Amoxicillin Alone) is Recommended for Empiric Antibiotic Treatment of Acute Bacterial Rhinosinusitis in Children (Strong Recommendation, Moderate Quality of Evidence)
Amoxicillin-Clavulanic Acid (Rather than Amoxicillin Alone) is Recommended for Empiric Antibiotic Treatment of Acute Bacterial Rhinosinusitis in Adults (Weak Recommendation, Low Quality of Evidence)
Dose: 500 mg/125 mg PO TID or 875 mg/125 mg PO BID
Pharmacology
Clavulanic Acid Enhances Coverage for Ampicillin-Resistant Haemophilus Influenzae and Moraxella Catarrhalis
The Evidence Supporting the Use of Clavulanic Acid in the Treatment of Acute Bacterial Rhinosinusitis is More Robust in Children than in Adults (Clin Infect Dis, 2012) [MEDLINE]
The Introduction of Conjugated Pneumococcal Vaccination in Children Has Increased the Percentage of Acute Bacterial Rhinosinusitis Cases Due to Haemophilus Influenzae with a Decrease in the Percentage of Cases Due to Streptococcal Pneumoniae
Pregnancy
Amoxicillin-Clavulanic Acid is Class B (Acceptable)
Indications for High-Dose Amoxacillin-Clavulanic Acid (2 g PO BID) to Cover Penicillin Non-Susceptible (PNS) Streptococcus Pneumoniae (Weak Recommendation, Moderate Quality of Evidence) (Clinical Infectious Diseases, 2012) [MEDLINE] (Otolaryngol Head Neck Surg, 2015) [MEDLINE]
Age <2 y/o or >65 y/o
Antibiotic Use within the Past Month
Comorbid Conditions (Diabetes Mellitus or Chronic Cardiac/Hepatic/Renal Disease)
Exposure to Daycare
Immunocompromised State
Hospitalization in Last 5 Days
Residence in Geographic Region where Penicillin Non-Susceptible (PNS) Streptococcus Pneumoniae Rates are >10%
Severe Infection (Systemic Toxicity, Fever >102°C, Concern for Suppurative Complications)
Doxycycline is an Appropriate Alternative Agent in the Setting of Penicillin Allergy (Strong Recommendation, Moderate Quality of Evidence) (Clinical Infectious Diseases, 2012) [MEDLINE]
Levofloxacin/Moxifloxacin are Alternative Agents in Patient with Penicillin Allergy (Strong Recommendation, Moderate Quality of Evidence) (Clinical Infectious Diseases, 2012) [MEDLINE]
However, Due to Concern that the Risk of Adverse Effects Outweighs the Benefit in the Treatment of Acute Bacterial Rhinosinusitis, Fluoroquinolones Should Only Be Used When Other Options are Not Feasible
Doses
Levofloxacin: 500-75o mg PO qday
Moxifloxacin: 400 mg PO qday
Pregnancy
Fluoroquinolones are Contraindicated in Pregnancy
Combination Third-Generation Oral Cephalosporin (Cefixime, Cefpodoxime) + Oral Clindamycin (see Cefixime, Cefpodoxime, and Clindamycin)
Combination Third-Generation Oral Cephalosporin (Cefixime, Cefpodoxime) + Oral Clindamycin is an Alternative Regimen in Adult Patient with Penicillin Allergy (with Non–Type I Hypersensitivity Reaction) or From Geographic Regions with High Endemic Rates of Penicillin Non-Susceptible (PNS Streptococcus Pneumoniae (Weak Recommendation, Moderate Quality of Evidence) (Clinical Infectious Diseases, 2012) [MEDLINE]
Doses
Cefixime: 400 mg PO qday
Cefpodoxime: 200 MG PO BID
Clindamycin: 300 mg q6hrs
Pharmacology
Addition of Clindamycin Improves Coverage for β-Lactam-Resistant Streptococcus Pneumoniae (Albeit with an Increased Risk of Clostridium Difficile Infection)
Macrolides (Clarithromycin/Azithromycin)/Trimethoprim-Sulfamethoxazole/Monotherapy with Second or Third-Generation Cephalosporins
These Agents are Not Recommended for Empiric Therapy (Strong Recommendation, Moderate Quality of Evidence) (Clinical Infectious Diseases, 2012) [MEDLINE]
Due to High Rates of Streptococcus Pneumoniae Resistance to Macrolides (>40%) and Trimethoprim-Sulfamethoxazole (50%)
Due to High Rates of Haemophilus Influenzae Resistance to Trimethoprim-Sulfamethoxazole (27%)
However, Azithromycin Might Be an Acceptable Alternative in a Pregnant Patient with Penicillin Allergy
Routine Coverage for Staphylococcus Aureus (Methicillin-Sensitive or Methicillin-Resistant) is Not Recommended (Strong Recommendation, Moderate Quality of Evidence) (Clinical Infectious Diseases, 2012) [MEDLINE]
Duration of Antibiotic Therapy
Clinical Efficacy
Studies Indicate that Antibiotics Achieve Bacterial Eradication by Day 3 (BMC Ear Nose Throat Disord, 2006) [MEDLINE] (Diagn Microbiol Infect Dis, 2007) [MEDLINE]
Meta-Analysis of Short vs Long Duration of Antibiotic Therapy for Acute Bacterial Sinusitis (Br J Clin Pharmacol, 2009) [MEDLINE]: n = 12 randomized trials
There was No Difference in Response/Relapse Rates Between Short Courses (3-7 Days) vs Longer Courses (6-10 Days) of Antibiotics
Recommendations (Infectious Diseases Society of America-IDSA Clinical Practice Guideline for Acute Bacterial Rhinosinusitis in Children and Adults) (Clinical Infectious Diseases, 2012) [MEDLINE]
In Adults with Uncomplicated Acute Bacterial Rhinosinusitis, the Recommended Duration of Therapy is 5–7 Days (Weak Recommendation, Low-Moderate Quality of Evidence)
In Children with Uncomplicated Acute Bacterial Rhinosinusitis, the Recommended Duration of Therapy is 10–14 Days (Weak Recommendation, Low-Moderate Quality of Evidence)
Recommendations (American Academy of Otolaryngology-Head and Neck Surgery Clinical Practice Guideline for Adult Sinusitis) (Otolaryngol Head Neck Surg, 2015) [MEDLINE]
If a Decision is Made to Treat Acute Bacterial Rhinosinusitis with Antibiotics, Amoxicillin with or without Clavulanic Acid Should Be First-LIne Therapy (For 5-10 Days) for Most Adults (Recommendation Based on Randomized Controlled Trials with Heterogeneity and Noninferiority Design with a Preponderance of Benefit Over Harm)
Expected Clinical Response and Assessment for Treatment Failure
Patients with Acute Bacterial Rhinosinusitis are Expected to Demonstrate a Clinical Response to Empiric Antibiotics within 3-5 Days, Since Bacterial Eradication Has Been Demonstrated to Occur by Day 3 (BMC Ear Nose Throat Disord, 2006) [MEDLINE] (Diagn Microbiol Infect Dis, 2007) [MEDLINE]
Older Adults and Patients with Comorbidities Resolve Acute Bacterial Rhinosinusitis More Slowly (Although There Should Still Be Some Improvement within the First 5 Days of Antibiotics)
Reasons for Treatment Failure
Inadequate Antibiotic Dosing
Non-Infectious Etiology
Resistant Pathogen
Structural Abnormality
Recommendations (Infectious Diseases Society of America-IDSA Clinical Practice Guideline for Acute Bacterial Rhinosinusitis in Children and Adults) (Clinical Infectious Diseases, 2012) [MEDLINE]
An Alternative Management Strategy is Recommended if Symptoms Worsen After 48–72 hrs of Initial Empiric Antibiotics or Fail to Improve Despite 3–5 Days of Initial Empiric Antibiotics (Strong Recommendation, Moderate Quality of Evidence)
Patients Who Clinically Worsen Despite 72 hrs of Antibiotics or Fail to Improve After 3–5 Days of Initial Empiric Antibiotics with a First-Line Agent Should Be Evaluated for the Possibility of Resistant Pathogens, a Noninfectious Etiology, Structural Abnormality, or Other Causes for Treatment Failure (Strong Recommendation, Low Quality of Evidence)
Trial of Second Course of Antibiotics
Suggested Agents (Use Different Drug Class for a Total of 7-10 Days)
Recommendations for Failure to Respond to Both First/Second-Line Antibiotics (i.e. Second Course of Antibiotics) (Infectious Diseases Society of America-IDSA Clinical Practice Guideline for Acute Bacterial Rhinosinusitis in Children and Adults) (Clinical Infectious Diseases, 2012) [MEDLINE]
In Patients with Acute Bacterial Rhinosinusitis Who Have Failed to Respond to Both First/Second-Line Antibiotics, It is Recommended that Cultures Be Obtained by Direct Sinus Aspiration Rather than By Nasopharyngeal Swab in Patients with Suspected Sinus Infection Who Have Failed to Respond to Empiric Antibiotics (Strong Recommendation, Moderate Quality of Evidence)
Nasopharyngeal Cultures are Unreliable and are Not Recommended for the Microbiologic Diagnosis of Acute Bacterial Rhinosinusitis (Strong Recommendation, High Quality of Evidence)
In Adults with Acute Bacterial Rhinosinusitis Who Have Failed to Respond to Both First/Second-Line Antibiotics, Endoscopically-Guided Cultures of the Middle Meatus May Be Considered (But Their Reliability in Children Has Not Been Established) (Weak Recommendation, Moderate Quality of Evidence)
Sinus Imaging (Sinus CT or Sinus MRI) are Recommended
Relapse After Treatment
Recurrence Within 2 wks of Response to Initial Treatment Usually Represents Inadequate Eradication of Infection
Patients with Good Response to Initial Therapy and Who Have Mild Symptoms of Relapse
Treat with a Longer Course of the Same Antibiotic
Patients Who Had Only Minimal Symptom Response with the Initial Antibiotic or Whose Relapse is Moderate to Severe
These Patients are More Likely to Have Organisms Resistant to the Initial Empiric Antibiotic and Require a Change in Antibiotic
Indications for Otolaryngology Referral
General Comments
Recommendations (Infectious Diseases Society of America-IDSA Clinical Practice Guideline for Acute Bacterial Rhinosinusitis in Children and Adults) (Clinical Infectious Diseases, 2012) [MEDLINE]
Patients Who are Seriously Ill and Immunocompromised, Continue to Clinically Deteriorate Despite Extended Courses of Antibiotics, or Have Recurrent Acute Rhinosinusitis (with Clearing Between Episodes) Should Be Referred to a Specialist (Otolaryngologist, Infectious Disease Specialist, or Allergist) for Consultation
Quantitative histology of the maxillary sinus. Rhinology. 1977;15(3):129 [MEDLINE]
Nosocomial sinusitis. JAMA 1982; 247:639-641
Upper respiratory tract infections in the critically ill. J Intensive Care Med 1990; 5:129-152
The evaluation of fever in the intensive care unit. Chest 1991; 100:213-220
Influence of long-term oro- or nasotracheal intubation on nosocomial maxillary sinusitis and pneumonia: results of a prospective, randomized, clinical trial. Crit Care Med 1993; 21:1132-1138
Principles of appropriate antibiotic use for acute rhinosinusitis in adults: background. Ann Intern Med. 2001 Mar 20;134(6):498-505 [MEDLINE]
Rhinosinusitis: establishing definitions for clinical research and patient care. J Allergy Clin Immunol 2004; 114:155 [MEDLINE]
Clinical practice guideline: adult sinusitis. Otolaryngol Head Neck Surg. 2007 Sep;137(3 Suppl):S1-31. doi: 10.1016/j.otohns.2007.06.726 [MEDLINE]
Effectiveness and safety of short vs. long duration of antibiotic therapy for acute bacterial sinusitis: a meta-analysis of randomized trials. Br J Clin Pharmacol. 2009;67(2):161 [MEDLINE]
In the clinic. Acute sinusitis. Ann Intern Med. 2010;153(5):ITC31 [MEDLINE]
IDSA clinical practice guideline for acute bacterial rhinosinusitis in children and adults. Infectious Diseases Society of America. Clin Infect Dis. 2012;54(8):e72 [MEDLINE]
European Position Paper on Rhinosinusitis and Nasal Polyps 2012. Rhinol Suppl. 2012 Mar;23:3 p preceding table of contents, 1-298 [MEDLINE]
Clinical practice guideline (update): adult sinusitis. Otolaryngol Head Neck Surg. 2015 Apr;152(2 Suppl):S1-S39 [MEDLINE]
Clinical Practice. Acute Sinusitis in Adults. N Engl J Med. 2016 Sep 8;375(10):962-70. doi: 10.1056/NEJMcp1601749 [MEDLINE]
Epidemiology
Summary health statistics for U.S. adults: national health interview survey, 2012. Vital Health Stat 10. 2014 Feb [MEDLINE]
Microbiology
Sinusitis of the maxillary antrum. N Engl J Med. 1975;293(15):735 [MEDLINE]
Role of the microbiota in immunity and inflammation. Cell. 2014;157(1):121 [MEDLINE]
The sinonasal bacterial microbiome in health and disease. Curr Opin Otolaryngol Head Neck Surg. 2016;24(1):20 [MEDLINE]
Physiology
Acute bacterial rhinosinusitis in adults: part I. Evaluation. Am Fam Physician. 2004;70(9):1685 [MEDLINE]
Diagnosis
Prevalence of incidental abnormalities on computed tomographic scans of the paranasal sinuses. Arch Otolaryngol Head Neck Surg. 1988;114(8):856 [MEDLINE]
Paranasal sinus bony anatomic variations and mucosal abnormalities: CT analysis for endoscopic sinus surgery. Laryngoscope. 1991;101(1 Pt 1):56 [MEDLINE]
Computed tomographic study of the common cold. N Engl J Med. 1994;330(1):25 [MEDLINE]
Role of middle meatus aspiration culture in the diagnosis of chronic sinusitis. Laryngoscope. 1997;107(12 Pt 1):1586 [MEDLINE]
Diagnosis and treatment of acute bacterial rhinosinusitis. Evid Rep Technol Assess (Summ). 1999 Mar;(9):1-5 [MEDLINE]
Endoscopically guided sinonasal cultures: a direct comparison with maxillary sinus aspirate cultures. Otolaryngol Head Neck Surg. 2000;122(3):370 [MEDLINE]
Rigid nasal endoscopy versus sinus puncture and aspiration for microbiologic documentation of acute bacterial maxillary sinusitis. Clin Infect Dis. 2001;33(10):1668 [MEDLINE]
Maxillary sinus puncture and culture in the diagnosis of acute rhinosinusitis: the case for pursuing alternative culture methods. Otolaryngol Head Neck Surg. 2002;127(1):7 [MEDLINE]
Endoscopy versus radiography for the diagnosis of acute bacterial rhinosinusitis. Eur Arch Otorhinolaryngol. 2005;262(5):416 [MEDLINE]
Endoscopically directed middle meatal cultures versus maxillary sinus taps in acute bacterial maxillary rhinosinusitis: a meta-analysis. Otolaryngol Head Neck Surg. 2006;134(1):3 [MEDLINE]
Clinical
Transmission of the common cold to volunteers under controlled conditions. 1 The common cold as a clinical entity. Arch Intern Med 1958; 101: 267–78 [MEDLINE]
Rhinovirus infections in an industrial population. II. Characteristics of illness and antibody response. JAMA. 1967;202(6):494 [MEDLINE]
Symptoms and signs of acute maxillary sinusitis. ORL J Otorhinolaryngol Relat Spec. 1976;38(5):298 [MEDLINE]
Comparison of subjective and radiological findings during the course of acute maxillary sinusitis. Ann Otol Rhinol Laryngol. 1983;92(1 Pt 1):75 [MEDLINE]
Histopathologic examination and enumeration of polymorphonuclear leukocytes in the nasal mucosa during experimental rhinovirus colds. Acta Otolaryngol Suppl 1984; 413: 19–24 [MEDLINE]
Analysis of symptoms and clinical signs in the maxillary sinus empyema. Acta Otolaryngol. 1988;105(3-4):343 [MEDLINE]
Clinical evaluation for sinusitis. Making the diagnosis by history and physical examination. Ann Intern Med. 1992;117(9):705 [MEDLINE]
The microbial etiology and antimicrobial therapy of adults with acute community-acquired sinusitis: a fifteen-year experience at the University of Virginia and review of other selected studies. J Allergy Clin Immunol. 1992;90(3 Pt 2):457 [MEDLINE]
Use of symptoms, signs, and blood tests to diagnose acute sinus infections in primary care: comparison with computed tomography. Fam Med. 1996;28(3):183 [MEDLINE]
Effect of oxymetazoline nose drops on acute sinusitis in the rabbit. Ann Otol Rhinol Laryngol. 1996;105(3):222 [MEDLINE]
The common cold. Prim Care. 1996;23(4):657 [MEDLINE]
Epidemiology, pathogenesis, and treatment of the common cold. Ann Allergy Asthma Immunol. 1997;78(6):531 [MEDLINE]
A practical guide for the diagnosis and treatment of acute sinusitis. CMAJ. 1997;156 Suppl 6:S1 [MEDLINE]
Parameters for the diagnosis and management of sinusitis. J Allergy Clin Immunol. 1998;102(6 Pt 2):S107 [MEDLINE]
The clinical diagnosis of acute purulent sinusitis in general practice–a review. Br J Gen Pract. 2002;52(479):491 [MEDLINE]
Effects of acetylsalicylic acid on sore throat pain and other pain symptoms associated with acute upper respiratory tract infection. Pain Med. 2003 Jun;4(2):118-24. doi: 10.1046/j.1526-4637.2003.03019.x [MEDLINE]
The common cold. Lancet. 2003;361(9351):51 [MEDLINE]
EAACI position paper on rhinosinusitis and nasal polyps executive summary. Allergy. 2005;60(5):583 [MEDLINE]
Understanding the symptoms of the common cold and influenza. Lancet Infect Dis. 2005;5(11):718 [MEDLINE]
How long does a cough last? Comparing patients’ expectations with data from a systematic review of the literature. Ann Fam Med. 2013;11(1):5 [MEDLINE]
No evidence for distinguishing bacterial from viral acute rhinosinusitis using symptom duration and purulent rhinorrhea: a systematic review of the evidence base. Otolaryngol Head Neck Surg. 2014;150(4):533 [MEDLINE]
No evidence for distinguishing bacterial from viral acute rhinosinusitis using fever and facial/dental pain: a systematic review of the evidence base. Otolaryngol Head Neck Surg. 2014;150(1):28 [MEDLINE]
Treatment
Management of respiratory problems in the aged. J Am Geriatr Soc. 1982;30(11 Suppl):S36 [MEDLINE]
CAFFS Trial. Comparison of cefuroxime with or without intranasal fluticasone for the treatment of rhinosinusitis. The CAFFS Trial: a randomized controlled trial. JAMA. 2001;286:3097-3105 [MEDLINE]
Intranasal flunisolide spray as an adjunct to oral antibiotic therapy for sinusitis. Clin Immunol. 2003;92:812-823 [MEDLINE]
Eradication of common pathogens at days 2, 3 and 4 of moxifloxacin therapy in patients with acute bacterial sinusitis. BMC Ear Nose Throat Disord. 2006;6:8 [MEDLINE]
Serial sinus aspirate samples during high-dose, short-course levofloxacin treatment of acute maxillary sinusitis. Diagn Microbiol Infect Dis. 2007;57(1):105 [MEDLINE]
Antibiotics and topical nasal steroid for treatment of acute maxillary sinusitis: a randomized controlled trial. JAMA. 2007;298:2487-2496 [MEDLINE]
Antibiotics for adults with clinically diagnosed acute rhinosinusitis: a meta-analysis of individual patient data. Lancet. 2008;371(9616):908 [MEDLINE]
Antibiotic prescribing for self limiting respiratory tract infections in primary care: summary of NICE guidance. BMJ. 2008;337:a437 [MEDLINE]
Comparison of antibiotics with placebo for treatment of acute sinusitis: a meta-analysis of randomised controlled trials. Lancet. 2008;8:543-552 [MEDLINE]
A 51-year-old woman with acute onset of facial pressure, rhinorrhea, and tooth pain: review of acute rhinosinusitis. JAMA. 2009;301(17):1798 [MEDLINE]
Moxifloxacin five-day therapy versus placebo in acute bacterial rhinosinusitis. Laryngoscope 2010; 120:1057 [MEDLINE]
Systemic corticosteroids for acute sinusitis. Cochrane Database Syst Rev. 2011 Dec 7;(12):CD008115. doi: 10.1002/14651858.CD008115.pub2 [MEDLINE] -Intranasal corticosteroids in management of acute sinusitis: a systematic review and meta-analysis. Ann Fam Med. 2012;10:241-249 [MEDLINE]
Systemic corticosteroid monotherapy for clinically diagnosed acute rhinosinusitis: a randomized controlled trial. CMAJ. 2012 Oct 2;184(14):E751-7. doi: 10.1503/cmaj.120430 [MEDLINE]
Antibiotics for clinically diagnosed acute rhinosinusitis in adults. Cochrane Database Syst Rev. 2012;10:CD006089 [MEDLINE]
Intranasal steroids for acute sinusitis. Cochrane Database Syst Rev. 2013 Dec 2;2013(12):CD005149. doi: 10.1002/14651858.CD005149.pub4 [MEDLINE]
Heated, humidified air for the common cold. Cochrane Database Syst Rev. 2013 Jun 4;(6):CD001728. doi: 10.1002/14651858.CD001728.pub5 [MEDLINE]
Avoid prescribing antibiotics in acute rhinosinusitis. BMJ. 2014;349:g5703 [MEDLINE]
Antibiotics for acute maxillary sinusitis in adults. Cochrane Database Syst Rev. 2014;11;CD000243 [MEDLINE]
Effectiveness of steam inhalation and nasal irrigation for chronic or recurrent sinus symptoms in primary care: a pragmatic randomized controlled trial. CMAJ. 2016;188(13):940 [MEDLINE]
Fatal Balamuthia mandrillaris brain infection associated with improper nasal lavage. Int J Infect Dis. 2018 Dec;77:18-22. doi: 10.1016/j.ijid.2018.09.013 [MEDLINE]
Antibiotics for acute rhinosinusitis in adults. Cochrane Database Syst Rev. 2018;9:CD006089 [MEDLINE]