Atelectasis is Defined as the Collapse of Aerated Lung
Etymology: Greek roots ateles and ektasis = incomplete expansion
Epidemiology
Atelectasis in the Intensive Care Unit (ICU) Setting
Incidence
Acute Lobar Atelectasis is One of the Commonly Encountered Clinical Problems in Critical Care Medicine (Chest, 2019) [MEDLINE]
Atelectasis (and Pulmonary Complications) in the Postoperative Setting
Lobar Atelectasis (to At Least Some Extent) May Complicate Many Major Surgeries (Eur J Radiol, 1996) [MEDLINE] (Current Opinion Anaesthesiology, 2007) [MEDLINE]
Lobar Atelectasis Occurs in 90% of Cardiac Surgeries
Lobar Atelectasis Occurs in 75% of Spinal Surgeries
Lobar Atelectasis Occurs in 25% of Upper Abdominal Surgeries
Postoperative Pulmonary Complications are a Major Etiology of Perioperative Morbidity and Mortality (Br J Anaesth, 2017) [MEDLINE]
General Risk Factors for Postoperative Pulmonary Complications (Am J Respir Crit Care Med, 2005) [MEDLINE] (Ann Intern Med, 2006) [MEDLINE] (J Clin Anesth, 2013) [MEDLINE]
Definite Risk Factors
Age >65 y/o
Chronic Obstructive Pulmonary Disease (COPD)
Cigarette Use within the Prior 8 wks
Active Tobacco Use Increases the Risk of Perioperative Pulmonary Complications (Although the Incremental Risk is Small in the Absence of Chronic Lung Disease)
Emergency Surgery
Functional Dependence
Heart Failure
Intraoperative Long-Acting Neuromuscular Blockade
Poor General Health Status (ASA Class >2)
Serum Albumin <3 g/dL
Surgery Lasting >3 hrs
Upper Abdominal/Thoracic (Open)/Aortic/Head and Neck/Neurosurgical/Abdominal Aortic Aneurysm Surgery
Probable Risk Factors
Abnormal Chest X-Ray
Arterial pCO2 >45 mm Hg
Current Upper Respiratory Tract Infection
General Anesthesia (as Compared to Spinal/Epidural Anesthesia or Other Regional Anesthesia)
Postoperative Nasogastric Tube Placement
ARISCAT Risk Index for Postoperative Pulmonary Complications (Anesthesiology, 2010) [MEDLINE]
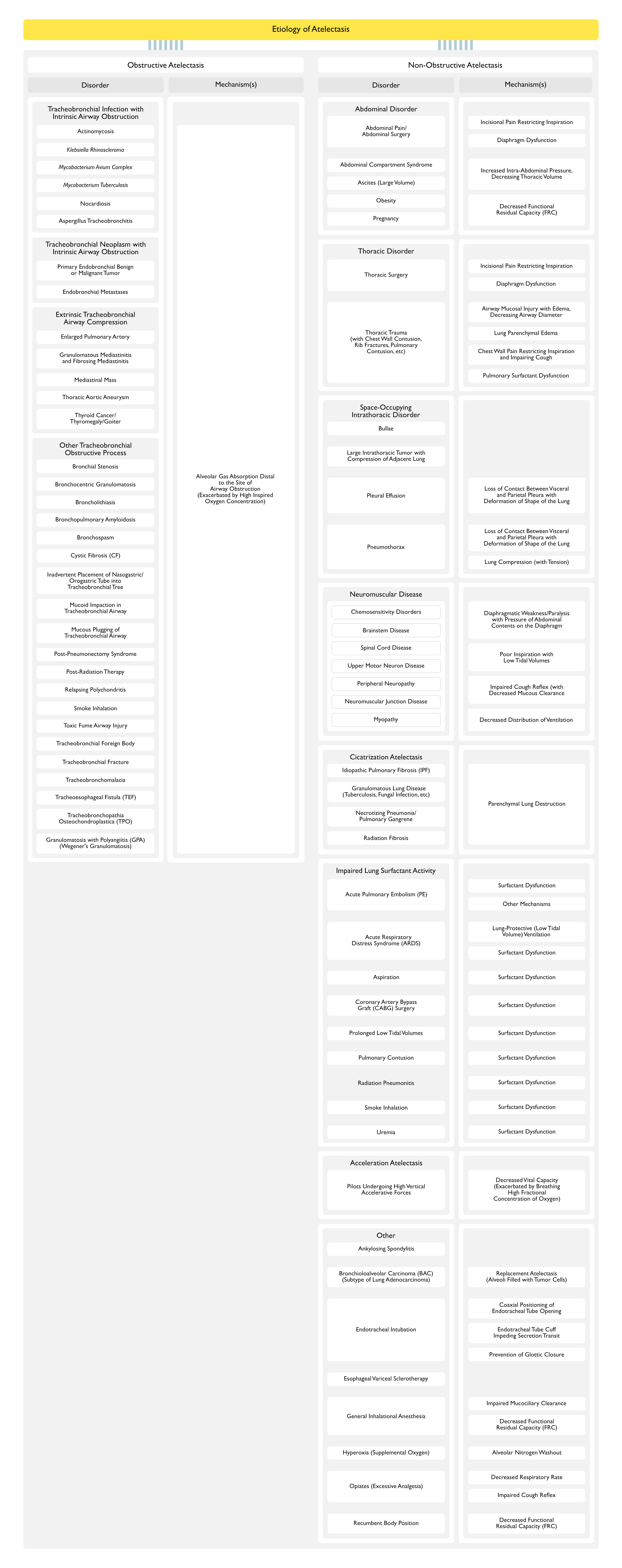
Airway Obstruction (of Any Etiology) Results in Absorptive Atelectasis Distal to the Site of Obstruction
Furthermore, High Inspired Oxygen Concentration (Which is Common in the Intensive Care Unit) Favors Alveolar Gas Absorption, Enhancing the Development of Atelectasis (J Appl Physiol, 2013) [MEDLINE]
Tracheobronchial Infection with Intrinsic Airway Obstruction
Atelectasis is Present in 5% of of Cystic Fibrosis Patients During the First 5 Years of Life (and Incidence Decreases with Aging) (Am Rev Respir Dis, 1978) [MEDLINE]
Atelectasis May Occur During an Exacerbation or without Other Clinical Symptoms
Physiology
Aspergillus-Associated Mucoid Impaction Can Be Etiologic in Some Cases (See Below) (Pediatr Radiol, 2007) [MEDLINE]
However, Most Cases Do Not Have a Demonstrable Mucoid Impaction on Bronchoscopy
Clinical
Atelectasis May Be Lobar or Segmental
Atelectasis Has a Right-Lung Predominance
Inadvertent Placement of Nasogastric/Orogastric Tube into Tracheobronchial Tree (see Nasogastric/Orogastric Tube)
Physiology
Inadvertent Placement of Nasogastric/Orogastric Tube into the Tracheobronchial Tree with Airway Obstruction
Mucoid Impaction in Tracheobronchial Airway (see Mucoid Impaction)
Mucoid Impaction is Common in Asthma (Especially in Patients with Poor Control)
While Bronchospasm Decreases Airway Diameter with Impaired Secretion Clearance, it Does Not Typically Result in Atelectasis without Simultaneous Mucous Plugging
Common Etiology of Airway Obstruction in the Intensive Care Unit
Associated with Bacterial Pneumonia (Particularly in a Patient with Other Risk Factors for Poor Secretion Clearance, Such as Altered Mental Status, Neuromuscular Disease, etc)
Abdominal Splinting is Common After Abdominal Surgery
Physiology
Incisional Pain Restricts Inspiration
Abdominal Surgery Impairs Diaphragmatic Activity
Diaphragmatic Activity During Expiration Normally Functions to Slow the Rate of Lung Deflation, Preventing Closure of Dependent Small Airways
Incisions in the Upper Abdomen or Lower/Midline Thorax Decrease Diaphragmatic Contractility (Regardless of Presence of Pain) (Am Rev Respir Dis, 1983) [MEDLINE]
In Contrast, Lower Abdominal Incisions (Laparoscopic Procedures, etc) Have a Very Limited Impact on Diaphragmatic Functioning (Arch Surg, 1993) [MEDLINE]
Increased Intra-Abdominal Pressure, Resulting in Decreased Thoracic Volume
Abdomen-Impeded Diaphragmatic Descent Decreases the Functional Residual Capacity (FRC)
In a Study of Sedated and Paralyzed Patients, Morbid Obesity Decreased the Functional Residual Capacity (FRC) and Increased the Alveolar-Arterial Oxygen (A-a O2) Gradient (J Appl Physiol, 1997) [MEDLINE]
Increased Intra-Abdominal Pressure, Resulting in Decreased Thoracic Volume
Abdomen-Impeded Diaphragmatic Descent Decreases the Functional Residual Capacity (FRC)
Thoracic Disorder
Thoracic Surgery
Physiology
Incisional Pain Restricts Inspiration
Thoracic Surgery Impairs Diaphragmatic Activity
Diaphragmatic Activity During Expiration Normally Functions to Slow the Rate of Lung Deflation, Preventing Closure of Dependent Small Airways
Incisions in the Upper Abdomen or Lower/Midline Thorax Decrease Diaphragmatic Contractility (Regardless of Presence of Pain) (Am Rev Respir Dis, 1983) [MEDLINE]
In Contrast, Lower Abdominal Incisions (Laparoscopic Procedures, etc) Have a Very Limited Impact on Diaphragmatic Functioning (Arch Surg, 1993) [MEDLINE]
Expansion of Bulla (Especially on Mechanical Ventilation), Resulting in Compression of Adjacent Lung
Due to Increased Compliance of the Bullous Lesion, Airflow on Mechanical Ventilation Tends to Be Redirected to the Bullous Lesion with Disproportionate Expansion of It (as Compared the Remaining Lung)
Large Intrathoracic Tumor with Compression of Adjacent Lung
Introduction of Air into Pleural Space Leads to Compression of Adjacent Lung (to Some Extent) and the Loss of Contact Between the Visceral and Parietal Surfaces with Deformation of Shape of Lung, Resulting in Atelectasis
Tension Pneumothorax
Mechanism Involves Positive Pressure in the Pleural Space with Compression of Adjacent Lung
ARDS is Associated with Decreased Surfactant Synthesis or Decreased Surfactant Activity, Resulting in Alveolar Instability and Collapse
Lung-Protective Low Tidal Volume Ventilation Used Commonly in the Treatment of ARDS May Predispose to the Development of Atelectasis (Respir Care, 2001) [MEDLINE]
May Occur During Lung-Protective Ventilation, Which is Used Commonly in the Mangement of Acute Respiratory Distress Syndrome (ARDS) (see Acute Respiratory Distress Syndrome)
Physiology
Persistently Low Tidal Volumes Predispose to Development of Atelectasis (Respir Care, 2001) [MEDLINE]
This Can Countered by Periodic Sighs and/or Positive End-Expiratory Pressure (PEEP)
Acceleration Atelectasis Has Been Described in Pilots Subjected to High, Vertical Accelerative Forces (Between 5-9G) (Aviat Space Environ Med, 1987) [MEDLINE]
At 5G, up to 50% of Pulmonary Airways are Distorted and/or Closed Due to Gravitational Forces
Physiology
Acceleration Atelectasis is Exacerbated by Breathing a High Fractional Concentration of Oxygen
Data from the I-LOCATE Trial Indicate that the Incidence of Atelectasis Developing During Bronchoscopy Performed Under General Anesthesia in Dependent Lung Zones is High (Occurred in 89% of Cases) (Chest, 2020) [MEDLINE]
Median Time from Anesthesia Induction to Development of Atelectasis: 33 min (Range: 3-94 min) (Chest, 2020) [MEDLINE]
The Degree of Atelectasis Which Occurs Following Bronchoscopy Performed Under General Anesthesia is Proportional to Body Mass Index and Length of General Anesthesia (Chest, 2020) [MEDLINE]
Physiology
General Inhalational Anesthesia Causes Atelectasis, Independent of Other Risk Factors (Such as Hyperoxia, Recumbent Position, Surgical Incisions, etc)
General Anesthesia Causes a Loss in Muscle Tone, Resulting in a Decrease in Functional Residual Capacity (FRC) (see General Anesthesia) (Best Pract Res Clin Anaesthesiol, 2010) [MEDLINE]
General Anesthesia Impairs the Mucociliary Escalator (Am Rev Respir Dis, 1976) [MEDLINE]
Hyperoxia (Excessive Oxygen Administration) (see Oxygen)
Epidemiology
Hyperoxia May Occur During Induction for General Anesthesia in the Preoperative Setting (Best Pract Res Clin Anaesthesiol, 2010) [MEDLINE]
Physiology
Hyperoxia Results in Washout of Nitrogen from Alveolus, Resulting in Oxygen Absorption from the Alveolus into the Blood, Leading to a Small Alveolus Which is Prone to Collapse (“Absorptive Atelectasis”)
Inhalation of 100% Oxygen During Anesthesia for Only 5 min Results in Atelectasis with Increased Intrapulmonary Right-to-Left Shunt (Anesthesiology, 2003) [MEDLINE]
At Moderate Doses, Opiates Tend to Preserve the Tidal Volume, But Decrease the Respiratory Rate (Which Predisposes to the Development of Atelectasis) (Anaesthesia, 1999) [MEDLINE] (Br J Anaesth, 2008) [MEDLINE]
Use of Excessive Analgesia During the Postoperative Period, etc Decreases Respiratory Drive and Impairs the Cough Reflex (Lung, 1981) [MEDLINE]
Recumbent Body Position
Mechanism
Recumbent Body Position Decreases the Functional Residual Capacity (FRC)
Healthy Adult Loses 700-1,200 mL of Functional Residual Capacity (FRC) in the Transition from Sitting to Fully Supine (Recumbent) Body Position (Am Rev Respir Dis, 1984) [MEDLINE]
In the Fully Supine Position, the Weight of the Heart and Mediastinum Narrow and Pinch the Left Lower Lobe Bronchi (Am J Respir Crit Care Med, 2000) [MEDLINE]
Physiology
Background
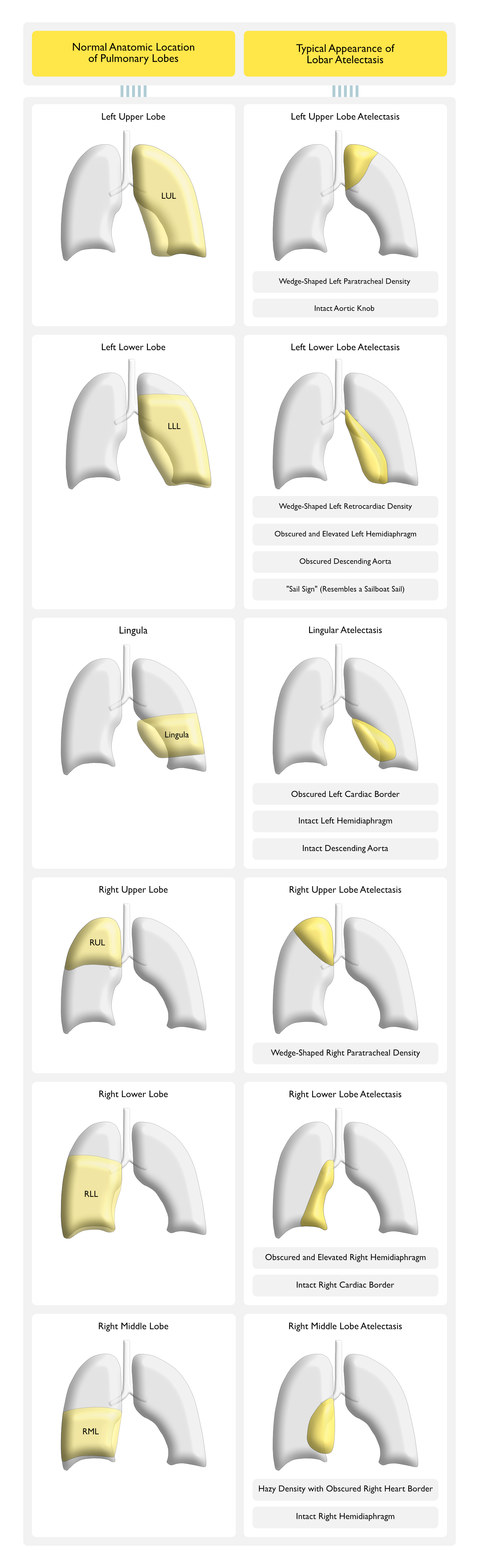
Normal Lobar Lung Anatomy
The Lung is Divided into Lobes by Fissures Which are Relatively Impermeable to Gas Transfer
This Anatomic Configuration Likely Serves to Compartmentalize Infection and Tissue Damage to a Smaller Region of the Lung (Crit Care Med, 2008) [MEDLINE]
However, Some Lung Fissures are Incomplete, Allowing Collateral Ventilation
Relative Frequency of the Laterality of Lower Lobe Atelectasis
Collapse of the Left Lower Lobe Occurs Approximately Twice as Commonly as Collapse of the Right Lower Lobe (Br J Radiol, 1983) [MEDLINE]
While the Right Mainstem Bronchus Has a Straighter Course than the Left Mainstem Bronchus, the Observed Increased Frequency of Left Lower Lobe Collapse is Likely Explained by Cardiac Compression and Deformation of Gravitationally-Dependent Bronchi (Am J Respir Crit Care Med, 2000) [MEDLINE]
Mechanical Determinants of the Functional Residual Capacity (FRC)
Functional Residual Capacity (FRC) is a Reflection of the Balance Between the Lung’s Tendency to Collapse and the Chest Wall’s Tendency to Expand
FRC is Typically Preserved or Increases with Aging (Clin Interv Aging, 2006) [MEDLINE]
Recumbent Body Position Significantly Decreases the FRC, Due to the Following Factors
The Positional Changes of Pressure and Volume are Most Pronounced Over the Range of 60° to 0° from Horizontal (Scand J Rehab Med, 1971) [MEDLINE]
Alterations of the Chest Wall Configuration
Hydrostatic Forces
Transpulmonary Pressures (Alveolar-Pleural Pressures) in the Dependent Regions of the Lung are Lower than Those in Superior Regions of the Lung
The Lung Volume at Which Closure of Dependent Airways Begins is Termed the Closing Volume
With Aging, the FRC May Decrease Below the Closing Volume (Especially in the Recumbent Body Position) (J Appl Physiol, 1970) [MEDLINE]
Role of Alveolar-Capillary Gas Exchange in Preventing Alveolar Collapse
During Normal Room Air Breathing, Venous Blood Flowing Past the Alveolus Has a pO2 Which is Approximately 50 mm Hg Below the Atmospheric pO2 (Due to the Normal Arteriovenous Oxgen Differential)
Maintaining the Pulmonary Capillary to Alveolus Diffusion Gradient (While Sustaining Alveolar Patency) Requires a Continuous Supply of Gas and Maintenance of Adequate Transpulmonary Pressure to Counter the Forces Which Favor Lung Recoil (i.e. Collapse)
Hyperoxia Results in Washout of Nitrogen from Alveolus, Resulting in Oxygen Absorption from the Alveolus into the Blood, Leading to a Small Alveolus Which is Prone to Collapse (“Absorptive Atelectasis”)
Inhalation of 100% Oxygen During Anesthesia for Only 5 min Results in Atelectasis with Increased Intrapulmonary Right-to-Left Shunt (Anesthesiology, 2003) [MEDLINE]
When Breathing 100% FIO2, Absorptive Collapse of a Lobe with Compromised Ventilation May Occur in <60 min, While Complete Absorption While Filled with Room Air May Require 12-24 hrs (J Appl Physiol, 2013) [MEDLINE]
Mechanisms of Atelectasis
Mechanism of Obstructive Atelectasis (Most Common Mechanism of Atelectasis)
Endobronchial Airway Obstruction (at Any Point Between the Trachea and Distal Airways), Resulting in Reabsorption of Alveolar Oxygen and Nitrogen (with Collapse of Previously Aerated Lung)
Rate of Development of Atelectasis Depends on the Degree of Obstruction (Complete vs Partial), Presence of Collateral Ventilation to the Affected Alveoli (Provided by the Pores of Kohn and Canals of Lambert), and Composition of the Inspired Gas
Stages
Early Stage: collapse of aerated lung within hours (volume loss), leading to V/Q mismatch (with resulting hypoxemia) and mediastinal shift toward the atelectatic side
Later Stage: filling of collapsed alveoli with cells and secretions (which may prevent complete collapse)
Late Stage: persistent obstruction, leading to infection, fibrosis, and/or bronchiectasis
Mechanism of Non-Obstructive Atelectasis
May Occur Due to a Space-Occupying Lesion in the Thorax with Compression of Adjacent Lung, Due to Loss of Surfactant (with Alveolar Collapse), Due to the Loss of Visceral-Parietal Pleural Contact (Due to Pleural Effusion, Pneumothorax), or Due to Replacement of Parenchymal Lung Tissue by Scarring or Infiltrative Disease
Middle and Lower Lobes Tend to Collapse More Readily in the Presence of Pleural Effusion
Upper lobes tend to collapse more readily in the presence of pneumothorax
Atelectasis Also Contributes to the Development of Pleural Effusion
Atelectasis (of Any Etiology) Creates Decreased Perimicrovascular Pressure, Resulting in Movement of Fluid from Parietal Pleural Interstitium into the Pleural Space (Until the Gradient Equalizes)
Consequences of Lobar Atelectasis
Impaired Global Lung Compliance with Increased Ventilatory Workload, Resulting in Hypoxemic, Hypercapnic Respiratory Failure (see Respiratory Failure)
Usually Small, Unilateral Pleural Effusion, with Associated Volume Loss (and Normal Heart Size)
Pleural Fluid is Typically Transudative in Cases of Effusion Which Occurs Secondary to Atelectasis (However, in Cases Where the Pleural Effusion is the Primary Event, Pleural Fluid May Be Either Transudative or Exudative)
Likely Occurs Due to Effects of General Anesthesia, Manipulation of the Lung, Diaphragmatic Dysfunction, Hypoventilation (Due to Pain), and/or Surfactant Dysfunction
Prevention
Recruitment Maneuver Followed by PEEP, May Together Decrease the Development of Atelectasis and Improved Oxygenation in Morbidly Obese Patients Undergoing General Anesthesia (Anesthesiology, 2009) [MEDLINE]
Lack of Association Between Atelectasis and Fever
Studies Do Not Indicate that There is a Correlation Between Atelectasis and Fever (Chest, 2011) [MEDLINE]
Middle Lobe Syndrome is Most Consistently Defined in the Medical Literature as Recurrent or Chronic Right Middle Lobe Atelectasis (see Atelectasis) (Postgrad Med, 1948) [MEDLINE] (Dis Chest, 1966) [MEDLINE] (Thorax, 1980) [MEDLINE] (Respiration, 2012) [MEDLINE]
A Similar Syndrome May Also Occur in the Lingula, Being Termed the “Lingula Syndrome” (Chest, 2004) [MEDLINE]
Etiology
Similar to Other Types of Atelectasis, Middle Lobe Syndrome Can Be Either Obstructive or Non-Obstructive
Clinical
Asymptomatic, Incidentally-Noted Right Middle Lobe Atelectasis on Chest X-Ray (CXR) or Chest Computed Tomography (CT) (see Chest X-Ray and Chest Computed Tomography)
In One Histopathologic Study of Right Middle Lobe Syndrome Cases Cured Surgically (n = 60), 60% Had Chronic Suppurative Infection, 33% Had Neoplasm, and 7% Had Tuberculosis (Med Interne, 1982) [MEDLINE]
Preoperative Exercise Program May Decrease the Risk of Postoperative Pulmonary Complications in Patients Undergoing Elective Lung, Cardiac or Abdominal Surgery (JAMA, 2006) [MEDLINE] (Clin Rehabil, 2011) [MEDLINE] (Cochrane Database Syst Rev, 2012) [MEDLINE] (Cochrane Database Syst Rev, 2015) [MEDLINE] (Eur J Vasc Endovasc Surg, 2015) [MEDLINE]
Australian Double-Blinded, Randomized Controlled Trial of Preoperative Chest Physical Therapy in the Prevention of Pulmonary Complications in Patients Undergoing Upper Abdominal Surgery (BMJ, 2018) [MEDLINE]: n = 441 adults
A 30 min Preoperative Physiotherapy and Breathing Exercise Training Session (within an Existing Hospital Multidisciplinary Preadmission Clinic) Halves the Incidence of Postoperative Pulmonary Complications and Specifically Hospital-Acquired Pneumonia
Intraoperative Measures
Utilize a Shorter Surgical Procedure (<3 hrs, If Possible)
Shorter Surgical Procedure Will Shorten the General Anesthesia Time
Utilize a Less Invasive Surgical Procedure (If Possible)
Types of Less Invasive Procedure (Assuming that Operative Time is Not Prolonged)
Laparoscopic Procedure
Robotic Procedure
Utilize Neuraxial Anesthesia (If Possible)
Neuraxial Anesthesia is Preferred Over General Anesthesia
Utilize Regional Anesthesia (If Possible)
Regional Anesthesia (Nerve Block) is Preferred, When This is an Option
Intraoperative Lung Protective Ventilation
International Expert Panel-Based Consensus Moderate to High-Quality Statements and Recommendations for Lung-Protective Ventilation for the Surgical Patient (Br J Anaesth, 2019) [MEDLINE]
Formation of Perioperative Clinically Significant Atelectasis May Be an Important Risk Factor for the Development of Postoperative Pulmonary Complications
Decreasing Lung/Chest Wall Compliance Caused by Surgical/Anaesthesia-Related Factors (i.e. Pneumoperitoneum, Positioning, and Circuit Disconnect) Should Be Treated by Appropriate Interventions
Individualized PEEP Can Prevent Progressive Alveolar Collapse
Recruitment Maneuvers Can Reverse Alveolar Collapse, But Have Limited Benefit without Sufficient PEEP
Increasing FIO2 May be Effective in Increasing the Oxygenation, But is Not an Effective Intervention to Improve Dynamic Compliance of the Respiratory System
Low Tidal Ventilation (6-8 ml/kg) and PEEP (+5 cm H2O) Should Be Used Initially (Zero PEEP is Not Recommended)
Appropriate PEEP and Recruitment Maneuvers May Improve Intraoperative Respiratory Function and Prevent Postoperative Pulmonary Complications
Before Anesthesia Induction, Position the Patient with the Head of Bed Elevated >30° (and Avoid Supine Positioning, If Possible)
If Not Contraindicated, Before the Loss of Spontaneous Ventilation, Use NIPPV or CPAP to Attenuate Anaesthesia-Induced Respiratory Changes
In Addition to Standard Monitoring, Dynamic Compliance, Driving Pressure (Plateau Pressure – PEEP) and Plateau Pressure Should Be Monitored on All Mechanically-Ventilated Patients
Continuous Hemodynamic and Oxygen Saturation Monitoring is Recommended Before and During the Performance of an Alveolar Recruitment Maneuver
Ensure Adequate Hemodynamic Stability Before Performing an Alveolar Recruitment Maneuver
Avoid Alveolar Recruitment Maneuvers when Contraindicated
For Patients with Asthma/Chronic Obstructive Pulmonary Disease (COPD), Administer Short-Acting β-Adrenergic Agonists (SABA’s) Prior to Intubation (see Asthma and Chronic Obstructive Pulmonary Disease)
Therapies
Administer SABA 2-4 Puffs within 30 min Prior to Intubation
Avoid Long-Active Neuromuscular Junction Antagonists During Induction and the Surgical Procedure (If Possible)
Avoid Swan-Ganz Catheter Placement (If Possible) (see Swan-Ganz Catheter)
Avoid Swan-Ganz Catheter Placement, Unless Required for the Procedure Itself (Such as For a Procedure Requiring Intraoperative Management of Congenital Heart Disease, Pulmonary Hypertension, etc)
Study of High-Flow Nasal Cannula vs Face Mask Oxygen in Patients Undergoing CT-Guided Hepatic Tumor Radiofrequency Ablation Under Deep Sedation (Eur J Anaesthesiol, 2020) [MEDLINE]
HFNC Oxygen Group Exhibited Les Postprocedural Atelectasis than the Face Mask Oxygen Group (Median 7.4 [Interquartile Range: 3.9-11.4%] vs 10.5 [Interquartile Range: 7.2-14.6%]; p = 0.0313)
The Number of Patients Requiring Oxygen Supplementation in the Recovery Room and During Transport from the Recovery Room to the Ward Did Not Differ Significantly Between the Groups (24.1 vs. 50.0%; p = 0.0596)
Ultrasound-Guided Lung Recruitment
Clinical Efficacy
Study of Ultrasound-Guided Lung Recruitment on the Development of Postoperative Atelectasis in Children Undergoing Simple Procedures (with Associated Endotracheal Intubation) (Eur J Anaesthesiol, 2020) [MEDLINE]
No Significant Difference Between the Groups, in Terms of Degree of Atelectasis as Assessed in the Post-Anesthesia Care Unit (PACU)
An Inspiratory Airway Pressure of >30 cm H2O was Required for Full Recruitment of Alveoli in Healthy Children
Study of Continuous Positive Airway Pressure to Prevent Postoperative Atelectasis in Anesthetized Children (Eur J Anaesthesiol., 2021) [MEDLINE]
Use of 5 cm H2O of CPAP in Healthy Children (Aged 6 mos-7 y/o) During Induction and Emergence of Anesthesia Prevented Atelectasis, with a Benefit Maintained During the First Postoperative Hour
Note that the Benefit is Greatest When Incentive Spirometry is Started Preoperatively
Clinical Efficacy
Systematic Review of Incentive Spirometry to Prevent Pulmonary Complications After CABG Surgery (Cochrane Database Syst Rev, 2007) [MEDLINE]: n = 4 trials (n = 443 patients)
Individual Small Trials Suggest No Evidence of Clinical Benefit of Incentive Spirometry in Decreasing Postoperative Pulmonary Complications and in Decreasing the Negative Effects on Pulmonary Function in Patients Who Have Undergone CABG
Patients Treated with Incentive Spirometry Had Worse Pulmonary Function and Arterial Oxygenation, as Compared to Positive-Pressure Breathing Modalities (CPAP, BiPAP, IPPB)
In View of the Modest number of Patients Studied, Methodological Shortcomings and Poor Reporting of the Included Trials, These Results Should Be Interpreted Cautiously
Systematic Review of Incentive Spirometry in Decreasing Pulmonary Complications in Patients Who Have Undergone Upper Abdominal Surgery (Cochrane Database Syst Rev, 2014)[MEDLINE]: n = 12 studies (n = 1834 patients)
Low-Quality Evidence Regarding the Lack of Efficacy of Incentive Spirometry for the Prevention of Postoperative Pulmonary Complications in Patients Who Have Undergone Upper Abdominal Surgery
Trial of Incentive Spirometry in Decreasing Pulmonary Complications in Patients Who Have Undergone Laparotomy (JAMA Surg, 2015) [MEDLINE]
Education and Incentive Spirometry for Unmonitored Patient Use Does Not Result in Statistically Significant Improvement in Pulmonary Dynamics Following Laparotomy
Intermittent positive pressure breathing (IPPB) was used commonly in the 1960s and 1970s, but was associated with more complications than other methods of lung expansion and is not part of routine management
Clinical Efficacy
IPPB is of Limited or No Value as Prophylaxis Against Postoperative Pulmonary Complications (Pneumonia, Atelectasis), as a Means of Delivering Aerosol Medications, or as a Means of Treating Stable Chronic Obstructive Pulmonary Disease (Postgrad Med, 1976) [MEDLINE]
Early Post-Operative Ambulation
Indicated for Postoperative Prevention of Atelectasis
Use of Epidural Anesthesia (Instead of Intravenous Opiates) is Preferred, When Applicable
Avoid Nonsteroidal Anti-Inflammatory Drugs (NSAID’s) (Such as Ketorolac, Ibuprofen, etc) in Patients with Asthma and/or Aspirin-Exacerbated Respiratory Disease (see Asthma and Aspirin-Exacerbated Respiratory Disease)
These Agents May Exacerbate Underlying Respiratory Disease
Continuous Positive Airway Pressure (CPAP)
Technique
Nasal or Full Face Mask CPAP at 10 cm H2O for 4-6 hrs
Clinical Efficacy
CPAP May Decrease the Incidence of Hypoxemia, Pneumonia, Reintubation, and ICU Admission in High-Risk Patients
Early Use of CPAP Via Mask for 30 min q2hrs Had Better Outcomes to Re-Open Collapsed Alveoli After Cardiac Surgery than Incentive Spirometry (Saudi Med J, 2012) [MEDLINE]
Systematic Review of CPAP in Perioperative Setting for Major Abdominal Surgery (Cochrane Database Syst Rev, 2014) [MEDLINE]
Very low-quality evidence from this review suggests that CPAP initiated during the postoperative period might reduce postoperative atelectasis, pneumonia and reintubation
Effects on mortality, hypoxia, and invasive ventilation were uncertain
Study of Continuous Positive Airway Pressure to Prevent Postoperative Atelectasis in Anesthetized Children (Eur J Anaesthesiol., 2021) [MEDLINE]
Use of 5 cm H2O of CPAP in Healthy Children (Aged 6 mos-7 y/o) During Induction and Emergence of Anesthesia Prevented Atelectasis, with a Benefit Maintained During the First Postoperative Hour
Avoiding Nasogastric Tubes Use After Abdominal Surgery (Unless Required for Symptom Control (see Nasogastric-Orogastric Tube)
Clinical Efficacy
Systematic Review of Nasogastric Tube Use Following Abdominal Surgery (Cochrane Database Syst Rev, 2005) [MEDLINE]
Routine Nasogastric Tube Use Does Not Accomplish Any of its Intended Goals and Should Be Abandoned in Favor of Selective Nasogastric Tube Use (to Specifically Treat Abdominal Distension or Nausea)
IPPB is of Limited or No Value as Prophylaxis Against Postoperative Pulmonary Complications (Pneumonia, Atelectasis), as a Means of Delivering Aerosol Medications, or as a Means of Treating Stable Chronic Obstructive Pulmonary Disease (Postgrad Med, 1976) [MEDLINE]
Treatment
General Measures
Treat Underlying Infection (If Present)
Antibiotics, as Required
Treat Underlying Conditions Which Might Impede Secretion Clearance (If Present)
Neuromuscular Disease/Neurologic Impairment
Humidification
Helps to Humidify Mucous
Upright Body Position
Rationale
Since Recumbent Body Position Decreases FRC and Enhances the Development of Atelectasis, Upright Body Position (and Mobilization) is Generally Recommended
Clinical Efficacy
Body Positioning is Generally More Effective as a Prophylactic Therapy when Combined with an Effective Secretion-Mobilizing Modality (Respir Care, 2012) [MEDLINE] (Burns, 2013) [MEDLINE]
Bronchodilators
Indications
Bronchodilators are Indicated for Patients with Airflow Obstruction
Systematic Review of Pharmacologic Agents (N-Acetylcysteine, Heparin + N-Acetylcysteine, Albuterol, Ipratropium Bromide, and Saline) Which Promote Airway Clearance in Hospitalized Subjects (Respir Care, 2015) [MEDLINE]: n = 9 studies (5 randomized controlled trials, 3 crossover randomized controlled trials, and 1 retrospective cohort study)
Studies Reported No Benefit of the Studied Agents on Expectoration, Pulmonary Function, and Atelectasis (and Little Effect on Changes in Sputum Volume, Weight, or Viscosity)
Standard Therapeutic Modality with Extensive Clinical Experience (J Thorac Dis, 2017) [MEDLINE]
Small Randomized Prospective Study of Therapeutic Bronchoscopy vs Chest Physical Therapy in the Treatment of Acute Lobar Atelectasis (Am Rev Respir Dis, 1979) [MEDLINE]: n = 31
No Significant Differences Between the Groups with Regard to Restoration of Volume Loss After the First Treatment Intervention, at 24 hrs, or at 48 hrs (p > 0.20)
Presence of Air Bronchogram was a Predictor of Delayed Resolution in Both Groups
At 24 hrs, 26% of the Air Bronchograms Demonstrated 83% Resolution (p < 0.001)
Narrative Review of Chest Physical Therapy in Mechanically-Ventilated Patients without Pneumonia ( J Thorac Dis, 2017) [MEDLINE]
Chest Physical Therapy was Safe, But Had Debatable or No Significant Impact on Any Relevant Patient Outcome Parameter (Including Pneumonia
Current Evidence Does Not Support Prophylactic Chest Physical Therapy in Adult Mechanically-Ventilated Patients without Pneumonia
Indicated for Significant Mucous Plugging with Associated Atelectasis (Particularly in Cases with Associated Respiratory Failure)
Small Randomized Prospective Study of Therapeutic Bronchoscopy vs Chest Physical Therapy in the Treatment of Acute Lobar Atelectasis (Am Rev Respir Dis, 1979) [MEDLINE]: n = 31
No Significant Differences Between the Groups with Regard to Restoration of Volume Loss After the First Treatment Intervention, at 24 hrs, or at 48 hrs (p > 0.20)
Presence of Air Bronchogram was a Predictor of Delayed Resolution in Both Groups
At 24 hrs, 26% of the Air Bronchograms Demonstrated 83% Resolution (p < 0.001)
RTX Respirator
Device
Biphasic External Cuirass-Style Ventilator
Clinical Efficacy
May Be Useful in Subset of Elderly Patients with Sputum Retention (Intern Med, 2009) [MEDLINE]
Retrospective Descriptive Study of the Effect of DNase on Atelectasis in Non-Cystic Fibrosis Pediatric Patients (Crit Care, 2005) [MEDLINE]
After Treatment with DNase for Atelectasis of Presumably Infectious Origin in Non-Cystic Fibrosis Pediatric Patients, Clinical Improvement was Observed within 2 hrs and Radiologic Improvement was Documented within 24 hrs in the Large Majority of Children
Increased Airway Obstruction and Ventilation-Perfusion Mismatch Occurred in 3 Children (Possibly Due to Rapid Mobilisation of Mucous)
Small Randomized Trial of Dornase Alfa vs Hypertonic Saline for the Treatment of Atelectasis in Mechanically-Ventilated Critically Ill Patients (J Aer Med Pulm Drug Del, 2012) [MEDLINE]: n = 33
No Significant Difference Between Dornase Alfa and Normal Saline (in Terms of Chest X-Ray Atelectasis Score)
No Significant Difference Between Hypertonic Saline and Normal Saline (in Terms of Chest X-Ray Atelectasis Score)
Australian Systematic Review of Inhaled Mucoactive Agents (Dornase Alfa, N-Acetylcysteine, Ambroxol, Hypertonic Saline, Heparin, Mannitol, and Isotonic Saline) in Critically Ill Medical/Surgical/Trauma Inpatients with Acute Lung Disease (Heart Lung, 2019) [MEDLINE]: n = 227 full-text articles were reviewed (of which 10 trials were included)
No Adverse Events were Reported for Dornase Alfa (n = 63), N-Acetylcysteine (N-Acetylcysteine, n = 50), Ambroxol (n = 140), Hypertonic Saline (n = 33), Heparin (n = 384), Mannitol (n = 20), or Isotonic Saline
During Invasive Mechanical Ventilation, N-Acetylcysteine, Dornase Alfa and Saline Had No Effect on Mucous
Postoperatively, Mucous Characteristics Improved with N-Acetylcysteine (n = 10)
Ambroxol Decrease Length of Stay (Mean Difference: 4 Days) and Halved Complications Following Lung Carcinoma Resection (n = 140)*
Heparin Improved Ventilator-Free Days (n = 130, Mean Difference 3.9-4.6 Days) and Intensive Care Length of Stay (n = 223, 3.2 Days), But Not Ventilator-Acquired Pneumonia
Dornase Alfa, Hypertonic Saline, and N-Acetylcysteine were Ineffective for Atelectasis/Mucous Plugging While Intubated
More Data are Required to Support Using N-Acetylcysteine, Ambroxol, and Heparin During Acute Illness
Induction of Osmotic Flow of Water into the Mucous Layer, Rehydrating the Airway Surface Liquid and Improving Mucociliary Clearance (J R Soc Med, 2011) [MEDLINE]
Decreases Airway Edema by Enhancing the Absorption of Water from the Mucosa and Submucosa
Disruption of Ionic Bonds within the Mucous Gel, Which Could Decrease Cross-Linking and Entanglements (J R Soc Med, 2011) [MEDLINE]
Dissociates DNA from the Mucoprotein, Which Allows Natural Proteolytic Enzymes to then Digest the Mucoprotein (J R Soc Med, 2011) [MEDLINE]
Decreases Pseudomonas Aeruginosa Biofilms (J R Soc Med, 2011) [MEDLINE]
Increase the Levels of the Antioxidants, Glutathione and Thiocyanate, in the Airway Surface Liquid (J R Soc Med, 2011) [MEDLINE]
Clinical Efficacy
Small Randomized Trial of Dornase Alfa vs Hypertonic Saline for the Treatment of Atelectasis in Mechanically-Ventilated Critically Ill Patients (J Aer Med Pulm Drug Del, 2012) [MEDLINE]: n = 33
No Significant Difference Between Dornase Alfa and Normal Saline (in Terms of Chest X-Ray Atelectasis Score)
No Significant Difference Between Hypertonic Saline and Normal Saline (in Terms of Chest X-Ray Atelectasis Score)
N-Acetylcysteine Liquefies Mucous and DNA Via Disruption of Disulfide Bonds
N-Acetylcysteine Has Antioxidant Effects (When Used at an Adequate Dose)
Clinical Efficacy
Systematic Review of Pharmacologic Agents (N-Acetylcysteine, Heparin + N-Acetylcysteine, Albuterol, Ipratropium Bromide, and Saline) Which Promote Airway Clearance in Hospitalized Subjects (Respir Care, 2015) [MEDLINE]: n = 9 studies (5 randomized controlled trials, 3 crossover randomized controlled trials, and 1 retrospective cohort study)
Studies Reported No Benefit of the Studied Agents on Expectoration, Pulmonary Function, and Atelectasis (and Little Effect on Changes in Sputum Volume, Weight, or Viscosity)
Australian Systematic Review of Inhaled Mucoactive Agents (Dornase Alfa, N-Acetylcysteine, Ambroxol, Hypertonic Saline, Heparin, Mannitol, and Isotonic Saline) in Critically Ill Medical/Surgical/Trauma Inpatients with Acute Lung Disease (Heart Lung, 2019) [MEDLINE]: n = 227 full-text articles were reviewed (of which 10 trials were included)
No Adverse Events were Reported for Dornase Alfa (n = 63), N-Acetylcysteine (N-Acetylcysteine, n = 50), Ambroxol (n = 140), Hypertonic Saline (n = 33), Heparin (n = 384), Mannitol (n = 20), or Isotonic Saline
During Invasive Mechanical Ventilation, N-Acetylcysteine, Dornase Alfa and Saline Had No Effect on Mucous
Postoperatively, Mucous Characteristics Improved with N-Acetylcysteine (n = 10)
Ambroxol Decrease Length of Stay (Mean Difference: 4 Days) and Halved Complications Following Lung Carcinoma Resection (n = 140)
Heparin Improved Ventilator-Free Days (n = 130, Mean Difference 3.9-4.6 Days) and Intensive Care Length of Stay (n = 223, 3.2 Days), But Not Ventilator-Acquired Pneumonia
Dornase Alfa, Hypertonic Saline, and N-Acetylcysteine were Ineffective for Atelectasis/Mucous Plugging While Intubated
More Data are Required to Support Using N-Acetylcysteine, Ambroxol, and Heparin During Acute Illness
Expert Review of Mucoactive Agents in Acutely Ill Patients (Expert Rev Respir Med, 2017) [MEDLINE]
In the Non-Cystic Fibrosis Patient Population, there is Limited Evidence Regarding these Medications
While Some Studies Have Found Benefit, the Quality of Evidence is Low
While Certain Patients May Derive Benefit, the General Use of these Medications in Acutely Ill Patients without Cystic Fibrosis Cannot Be Recommended at This Time
Substudy of Routine vs On-Demand Nebulization of N-Acetylcysteine with Salbutamol on the Accumulation of Airway Secretions in Endotracheal Tubes (Substudy of the NEBULAE Trial) (Intensive Care Med Exp, 2020) [MEDLINE]
In Adult Critically Ill Patients on Invasive Ventilation, Routine Nebulization of Mucolytics and Bronchodilators Did Not Affect Accumulation of Airway Secretions in the Endotracheal Tube
Utilization of Positive End-Expiratory Pressure (PEEP)
Study of Transpulmonary Pressure and Positive End-Expiratory Pressure in Morbidly Obese Patients (BMI 48 ± 11 kg/m2) (Crit Care Med, 2017) [MEDLINE]
In Morbid Obesity, Low-to-Negative Transpulmonary Pressures Predict Lung Collapse and Intratidal Recruitment/Derecruitment
After the Development of Atelectasis, Lung Recruitment Followed by a Decremental PEEP Trial Identified the PEEP Level (17.4 ± 2.1 cm H2O) Required to Restore Nonaerated Lung Tissue and Reestablish Lung Elastance and Oxygenation (While Avoiding Increased Pulmonary Vascular Resistance)
AARC Guideline for Pharmacologic Airway Clearance Therapies in Hospitalized Patients (Respir Care, 2015) [MEDLINE]
Hospitalized Adult and Pediatric Patients Without Cystic Fibrosis
Dornase Alfa is Not Recommended in Adults and Children with Non-Cystic Fibrosis Bronchiectasis
Routine Use of Bronchodilators to Aid in Secretion Clearance is Not Recommended
Routine Use of Aerosolized N-Acetylcysteine to Improve Airway Clearance is Not Recommended
Adult and Pediatric Patients With Neuromuscular Disease, Respiratory Muscle Weakness, or Impaired Cough
Due to Insufficient Evidence, Use of Aerosolized Agents to Change Sputum Physical Properties or Improve Airway Clearance is Not Recommended for Patients with Neuromuscular Disease or Weakness
Postoperative Adult and Pediatric Patients
Due to Insufficient Evidence, Mucolytics are Not Recommended in the Treatment of Atelectasis
Routine Administration of Bronchodilators to Postoperative Patients is Not Recommended
Prognosis/Complications
Complications of Re-Expansion of Atelectatic Lobe
Re-Expansion Pulmonary Edema May Occur Following Reinflation of a Long-Collapsed and Surfactant-Depleted Lung Lobe (J Appl Physiol Respir Environ Exerc Physiol, 1979) [MEDLINE] (Ann Thorac Cardiovasc Surg, 2008) [MEDLINE]
References
Effects of age and body position on “airway closure” in man. J Appl Physiol. 1970;28(4):448-451 [MEDLINE]
Effects of respiratory paralysis in tetraplegic and paraplegic patients. Scand J Rehab Med. 1971;3(4):145-150 [MEDLINE]
Influence of head-dependent positions on lung volume and oxygen saturation in chronic airflow obstruction. Am Rev Respir Dis. 1984;129:101-105 [MEDLINE]
Induction and prevention of acceleration atelectasis. Aviat Space Environ Med. 1987;58(1):69 [MEDLINE]
Residual curarisation: a comparative study of atracurium and pancuronium. Acta Anaesthesiol Scand. 1988;32(2):79 [MEDLINE]
Diaphragm function is not impaired by pneumoperitoneum after laparoscopy. Arch Surg. 1993;128(4):430-432 [MEDLINE]
Respiratory system mechanics in sedated, paralyzed, morbidly obese patients. J Appl Physiol. 1997;82(3):811-818 [MEDLINE]
Time course of changes in breathing pattern in morphine and oxycodone induced respiratory depression. Anaesthesia. 1999;54(9):835-840 [MEDLINE]
The prone position eliminates compression of the lungs by the heart. Am J Respir Crit Care Med. 2000;161(5):1660-1665 [MEDLINE]
Lung collapse during low tidal volume ventilation in acute respiratory distress syndrome. Respir Care. 2001;46(5): 489-490 [MEDLINE]
Endobronchial actinomycosis associated with foreign body: four cases and a review of the literature. Chest. 2002 Jun;121(6):2069-72. doi: 10.1378/chest.121.6.2069 [MEDLINE]
Optimal oxygen concentration during induction of general anesthesia. Anesthesiology. 2003 Jan;98(1):28-33 [MEDLINE]
DNase and atelectasis in non-cystic fibrosis pediatric patients. Crit Care. Aug 2005;9(4):R351-6 [MEDLINE]
Preoperative pulmonary risk stratification for noncardiothoracic surgery: systematic review for the American College of Physicians. Ann Intern Med. 2006;144(8):581 [MEDLINE]
Preoperative intensive inspiratory muscle training to prevent postoperative pulmonary complications in high-risk patients undergoing CABG surgery: a randomized clinical trial. JAMA. 2006;296(15):1851 [MEDLINE]
High-attenuation mucus plugs on MDCT in a child with cystic fibrosis: potential cause and differential diagnosis. Pediatr Radiol, 2007. 37:592-595 [MEDLINE]
Atelectasis in the perioperative patient. Curr Opin Anaesthesiol. 2007 Feb;20(1):37-42. doi: 10.1097/ACO.0b013e328011d7e5 [MEDLINE]
Reexpansion pulmonary edema. Ann Thorac Cardiovasc Surg. 2008;14(4):205-209 [MEDLINE]
Propagation prevention: a complementary mechanism for lung protective ventilation in ARDS. Crit Care Med. 2008;36(12):3252-3258 [MEDLINE]
Opioids and the control of respiration. Br J Anaesth. 2008;100(6):747-758 [MEDLINE]
Prevention of atelectasis in morbidly obese patients during general anesthesia and paralysis: a computerized tomography study. Anesthesiology. Nov 2009;111(5):979-87 [MEDLINE]
Lung surfactant alterations in pulmonary thromboembolism. Eur J Med Res. 2009 Dec 7;14 Suppl 4(Suppl 4):38-41. doi: 10.1186/2047-783x-14-s4-38 [MEDLINE]
Marked improvement of extensive atelectasis by unilateral application of the RTX respirator in elderly patients. Intern Med. 2009;48(16):1419-23 [MEDLINE] -Prediction of postoperative pulmonary complications in a population-based surgical cohort. Anesthesiology. 2010 Dec;113(6):1338-50. doi: 10.1097/ALN.0b013e3181fc6e0a [MEDLINE]
Mechanisms of atelectasis in the perioperative period. Best Pract Res Clin Anaesthesiol. 2010 Jun;24(2):157-69. doi: 10.1016/j.bpa.2009.12.002 [MEDLINE]
Effect of preoperative smoking cessation interventions on postoperative complications. J Am Coll Surg. 2011;212(6):1094 [MEDLINE]
Stopping smoking shortly before surgery and postoperative complications: a systematic review and meta-analysis. Arch Intern Med. 2011;171(11):983 [MEDLINE]
Smoking cessation reduces postoperative complications: a systematic review and meta-analysis. Am J Med. 2011;124(2):144 [MEDLINE]
Atelectasis as a cause of postoperative fever: where is the clinical evidence?. Chest. Aug 2011;140(2):418-24 [MEDLINE]
Mechanisms and applications of hypertonic saline. J R Soc Med. 2011 Jul; 104(Suppl 1): S2–S5 [MEDLINE]
The effects of preoperative exercise therapy on postoperative outcome: a systematic review. Clin Rehabil. 2011 Feb;25(2):99-111 [MEDLINE]
Preoperative physical therapy for elective cardiac surgery patients. Cochrane Database Syst Rev. 2012;11:CD010118 [MEDLINE]
Dornase alpha compared to hypertonic saline for lung atelectasis in critically ill patients. J Aer Med Pulm Drug Del. 2012;25(6):342-348. [MEDLINE]
A randomized trial of conventional chest physical therapy versus high frequency chest wall compressions in intubated and non-intubated adults. Respir Care. 2012;57(2):221-228 [MEDLINE]
Difference between continuous positive airway pressure via mask therapy and incentive spirometry to treat or prevent post-surgical atelectasis. Saudi Med J. 2012;33(11): 1190-1195 [MEDLINE]
Chest physiotherapy using intrapulmonary percussive ventilation to treat persistent atelectasis in hypoxic patients after smoke inhalation. Burns. 2013;39(1):192-193 [MEDLINE]
Reabsorption atelectasis in a porcine model of ARDS: regional and temporal effects of airway closure, oxygen, and distending pressure. J Appl Physiol. 2013;115(10):1464-1473 [MEDLINE]
Risk factors for predicting postoperative complications after open infrarenal abdominal aortic aneurysm repair: results from a single vascular center in China. J Clin Anesth. 2013;25(5):371 [MEDLINE]
Continuous positive airway pressure (CPAP) during the postoperative period for prevention of postoperative morbidity and mortality following major abdominal surgery. Cochrane Database Syst Rev. 2014 Aug 1;2014(8):CD008930. doi: 10.1002/14651858.CD008930.pub2 [MEDLINE]
Incentive spirometry for prevention of postoperative pulmonary complications in upper abdominal surgery. Cochrane Database Syst Rev. 2014 Feb 8;2014(2):CD006058. doi: 10.1002/14651858.CD006058.pub3 [MEDLINE]
Current challenges in the recognition, prevention and treatment of perioperative pulmonary atelectasis. Exp Rev Repir Med. 2015 Feb;9(1):97-107. doi: 10.1586/17476348.2015.996134 [MEDLINE]
The effect of incentive spirometry on postoperative pulmonary function following laparotomy: a randomized clinical trial. JAMA Surg. 2015;150(3):229-236 [MEDLINE]
AARC Clinical Practice Guideline: Effectiveness of Pharmacologic Airway Clearance Therapies in Hospitalized Patients. Respir Care. 2015 Jul;60(7):1071-7. doi: 10.4187/respcare.04165 [MEDLINE]
Preoperative inspiratory muscle training for postoperative pulmonary complications in adults undergoing cardiac and major abdominal surgery. Cochrane Database Syst Rev. 2015 Oct 5;(10):CD010356. doi: 10.1002/14651858.CD010356.pub2 [MEDLINE]
Beneficial Effects of Pre-operative Exercise Therapy in Patients with an Abdominal Aortic Aneurysm: A Systematic Review. Eur J Vasc Endovasc Surg. 2015;49(1):66 [MEDLINE]
Pharmacologic Agents That Promote Airway Clearance in Hospitalized Subjects: A Systematic Review. Respir Care. 2015 Jul;60(7):1061-70. doi: 10.4187/respcare.04086 [MEDLINE]
Transpulmonary pressure describes lung morphology during decremental positive end- expiratory pressure trials in obesity. Crit Care Med. 2017;45(8): 1374-1381 [MEDLINE]
Chest physiotherapy in mechanically ventilated patients without pneumonia—a narrative review. J Thorac Dis. 2017;9(1):E44-E49 [MEDLINE]
Effect of chest physiotherapy in patients undergoing mechanical ventilation: a prospective randomized controlled trial. Chin Crit Care Med. 2017;29(5):403-406 [MEDLINE]
The use of pulmonary clearance medications in the acutely ill patient. Expert Rev Respir Med. 2017 Oct;11(10):815-826. doi: 10.1080/17476348.2017.1358089 [MEDLINE]
The use of high frequency percussive ventilation after cardiac surgery significantly improves gas exchange without impairment of hemodynamics. Can J Respir Ther. 2018;54(3):58-61 [MEDLINE]
Preoperative physiotherapy for the prevention of respiratory complications after upper abdominal surgery: pragmatic, double blinded, multicentre randomised controlled trial. BMJ. 2018;360:5916 [MEDLINE]
Mucolytic agents versus placebo for chronic bronchitis or chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2019;5:CD001287 [MEDLINE]
Mucoactive agents for adults with acute lung conditions: A systematic review. Heart Lung. Mar-Apr 2019;48(2):141-147. doi: 10.1016/j.hrtlng.2018.09.010 [MEDLINE]
Acetylcysteine for Patients Requiring Secretion Clearance: A Review of Guidelines. CADTH Rapid Response Report: Summary with Critical Appraisal. 2019. [MEDLINE]
Lung-protective ventilation for the surgical patient: international expert panel-based consensus recommendations. Br J Anaesth. 2019 Dec;123(6):898-913. doi: 10.1016/j.bja.2019.08.017 [MEDLINE]
Incidence and Location of Atelectasis Developed During Bronchoscopy Under General Anesthesia: The I-LOCATE Trial. Chest. 2020 Dec;158(6):2658-2666. doi: 10.1016/j.chest.2020.05.565 [MEDLINE]
Airway closure, more harmful than atelectasis in intensive care? Intensive Care Med. 2020 Dec;46(12):2373-2376. doi: 10.1007/s00134-020-06144-w [MEDLINE]
Effects of high-flow nasal oxygen during prolonged deep sedation on postprocedural atelectasis: A randomised controlled trial. Eur J Anaesthesiol. 2020 Nov;37(11):1025-1031. doi: 10.1097/EJA.0000000000001324 [MEDLINE]
Effect of an ultrasound-guided lung recruitment manoeuvre on postoperative atelectasis in children: A randomised controlled trial. Eur J Anaesthesiol. 2020 Aug;37(8):719-727. doi: 10.1097/EJA.0000000000001175 [MEDLINE]
Perioperative interventions for prevention of postoperative pulmonary complications: systematic review and meta-analysis. BMJ. 2020 Mar 11;368:m540. doi: 10.1136/bmj.m540 [MEDLINE]
Effect of routine vs on-demand nebulization of acetylcysteine with salbutamol on accumulation of airway secretions in endotracheal tubes: substudy of a randomized clinical trial. Intensive Care Med Exp. 2020 Dec 18;8(Suppl 1):71. doi: 10.1186/s40635-020-00351-x [MEDLINE]
Prevention of atelectasis by continuous positive airway pressure in anaesthetised children: A randomised controlled study. Eur J Anaesthesiol. 2021 Jan;38(1):41-48. doi: 10.1097/EJA.0000000000001351 [MEDLINE]
Feasibility and safety of intrapulmonary percussive ventilation in spontaneously breathing, non-ventilated patients in critical care: A retrospective pilot study. J Intensive Care Soc. 2021 May;22(2):111-119. doi: 10.1177/1751143720909704 [MEDLINE]