Preeclampsia: new onset of hypertension and proteinuria or hypertension and end-organ dysfunction with/without proteinuria after 20 was of gestation in a previously normotensive female
Preeclampsia May Also Develop Postpartum in Some Cases
Eclampsia: preeclampsia with seizures (without an alternative neurologic explanation for the seizures)
Demographics
Incidence: occurs in approximately 4.6% of pregnancies worldwide
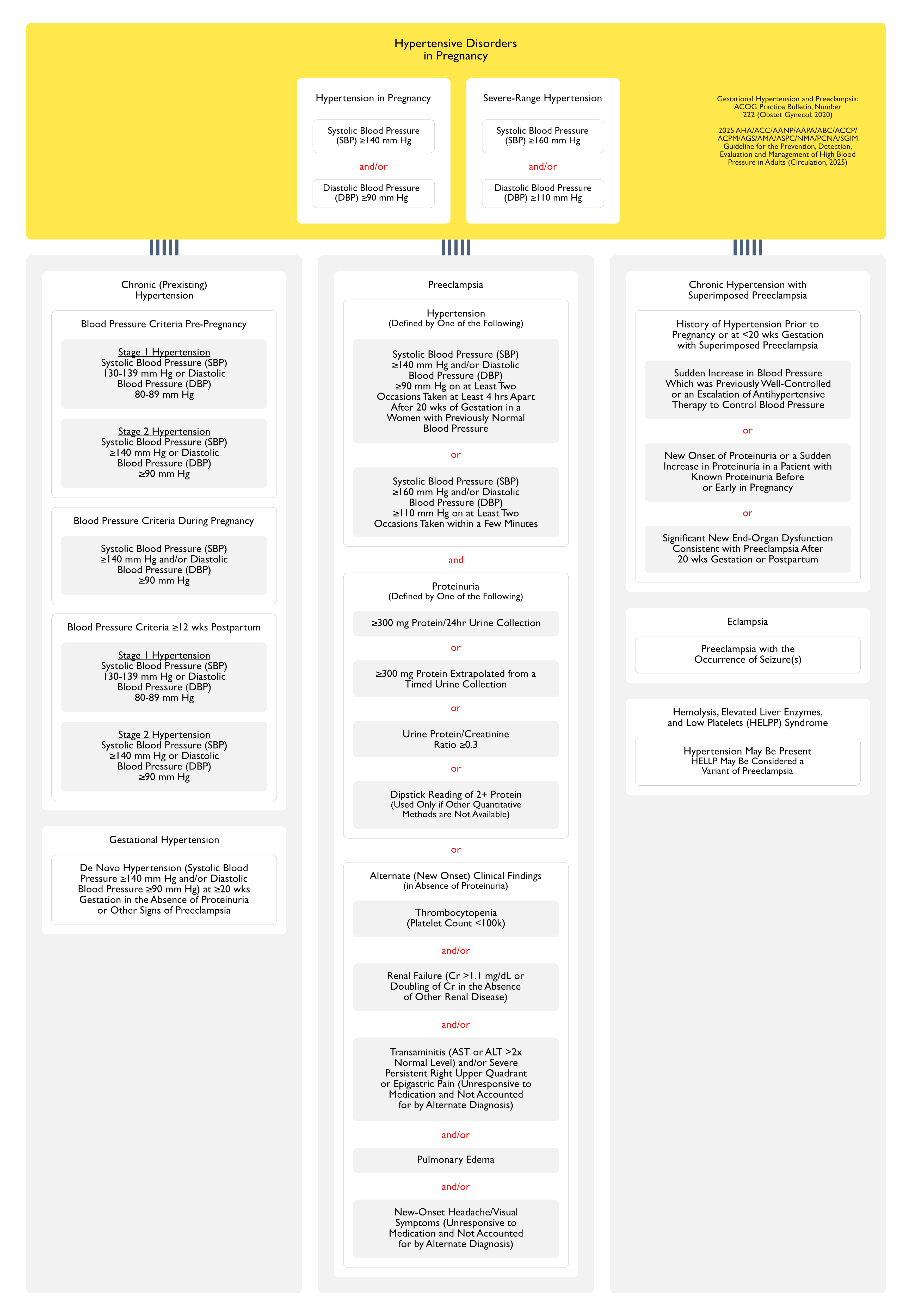
Diagnostic Criteria for Preeclampsia (One of the Following) (Obstet Gynecol, 2013) [MEDLINE]
Systolic Blood Pressure ≥140 mm Hg or Diastolic Blood Pressure ≥90 mm Hg on Two Occasions at Least Four Hours Apart After 20 wks of Gestation in a Previously Normotensive Patient
New-Onset Hypertension with the New Onset of Any of the Following (with/without Proteinuria)
Platelet Count <100k
Serum Creatinine >1.1 mg/dL or Doubling of the Serum Creatinine in the Absence of Other Renal Disease
Liver Transaminases at Least 2x the Upper Limit of Normal
Pulmonary Edema
Cerebral/Visual Symptoms
New-Onset or Persistent Headaches Unresponsive to Usual Doses of Analgesics
Severe Headache/Headache Unresponsive to Analgesic Therapy
New-Onset Visual Symptoms
Cortical Blindness
Photophobia
Retinal Vasospasm
Scotomata
Hepatic Abnormality
Severe Persistent RUQ/Epigastric Pain Unresponsive to Analgesia (Not Due to Another Diagnosis) or Transaminases ≥2x Upper Limit of Normal
Severe Hypertension
Systolic Blood Pressure ≥160 mm Hg or Diastolic Blood Pressure ≥110 mm Hg on Two Occasions at Least 4 hrs Apart While the Patient is on Bedrest: antihypertensive therapy can be initiated on confirmation of severe hypertension without waiting for 4 hrs to elapse
Thrombocytopenia (Platelet Count <100k)
Renal Abnormality with Progressive Renal Failure
Serum Cr >1.1 mg/dL or Doubling of Serum Cr in Absence of Other Renal Disease
Pulmonary Edema
Therapy
Delivery
Alternately, Conservative Management Can Be Used for Select Cases ≥24 wks and <34 wks of Gestation
Prognosis
XXXXX
xxxx
References
Hypertension in pregnancy. Report of the American College of Obstetricians and Gynecologists’ Task Force on Hypertension in Pregnancy. Obstet Gynecol. 2013 Nov;122(5):1122-31. doi: 10.1097/01.AOG.0000437382.03963.88 [MEDLINE]