Nonexpandable Lung is Defined as a Lung Unable to Expand to the Chest Wall and Achieve Visceral and Parietal Pleural Apposition (Am J Med Sci, 2008) [MEDLINE] (F1000 Med Rep, 2010) [MEDLINE]
Factors Contributing to Nonexpandable Lung (F1000 Med Rep, 2010) [MEDLINE]
Fibrotic Processes Affecting the Visceral Pleura
Extrapleural Processes (Such as Endobronchial Obstruction, Chronic Lung Atelectasis, etc)
Processes Which Increase the Elastic Recoil of the Lung (Such as Interstitial Lung Disease, Lymphangitic Carcinomatosis, etc)
Types of Nonexpandable Lung
Lung Entrapment
Lung Entrapment is Defined as the Inability for the Lung to Expand Fully Because of an Active Disease (Such as Infection or Malignancy Which Restricts Lung and/or Visceral Pleural Expansion)
Pleural Fluid is Usually an Exudate
Most Cases of Lung Entrapment Resolve (with Resolution of the Inflammatory Process)
However, in Some Cases, the Resolution May Be Incomplete, Resulting in Trapped Lung
In This Respect, Lung Entrapment and Trapped Lung Represent Different Points on a Continuum of the Same Disease Process
Trapped Lung
Trapped Lung is Defined as Inability for the Lung to Expand Fully Because of a Remote Inflammatory Condition Which Has Left a Residual Collagenous/Fibrous Peel on the Visceral Pleura
Pleural Fluid is Usually a Transudate or a Protein-Discordant Exudate
Pleural Fluid is Usually Mononuclear Cell-Predominant
Most Cases of Trapped Lung Begin as a Form of Lung Entrapment
Epidemiology
Incidence
In Patients Undergoing Thoracentesis, Approximately 10% Have Nonexpandable Lung
Approximately 20% of Patients Undergoing Therapeutic Thoracentesis Have Nonexpandable Lung
Approximately 30% of Patients Undergoing Therapeutic Thoracentesis for Malignant Pleural Effusion Have Nonexpandable Lung
Pleural Fluid Accumulation is Due to Increased Elastic Recoil of an Atelectatic/Consolidated Lung and Increased Pleural Fluid Production by the Visceral Pleura
In Contrast to Malignancy, Decreased Parietal Pleural Drainage Does Not Appear to Be a Factor
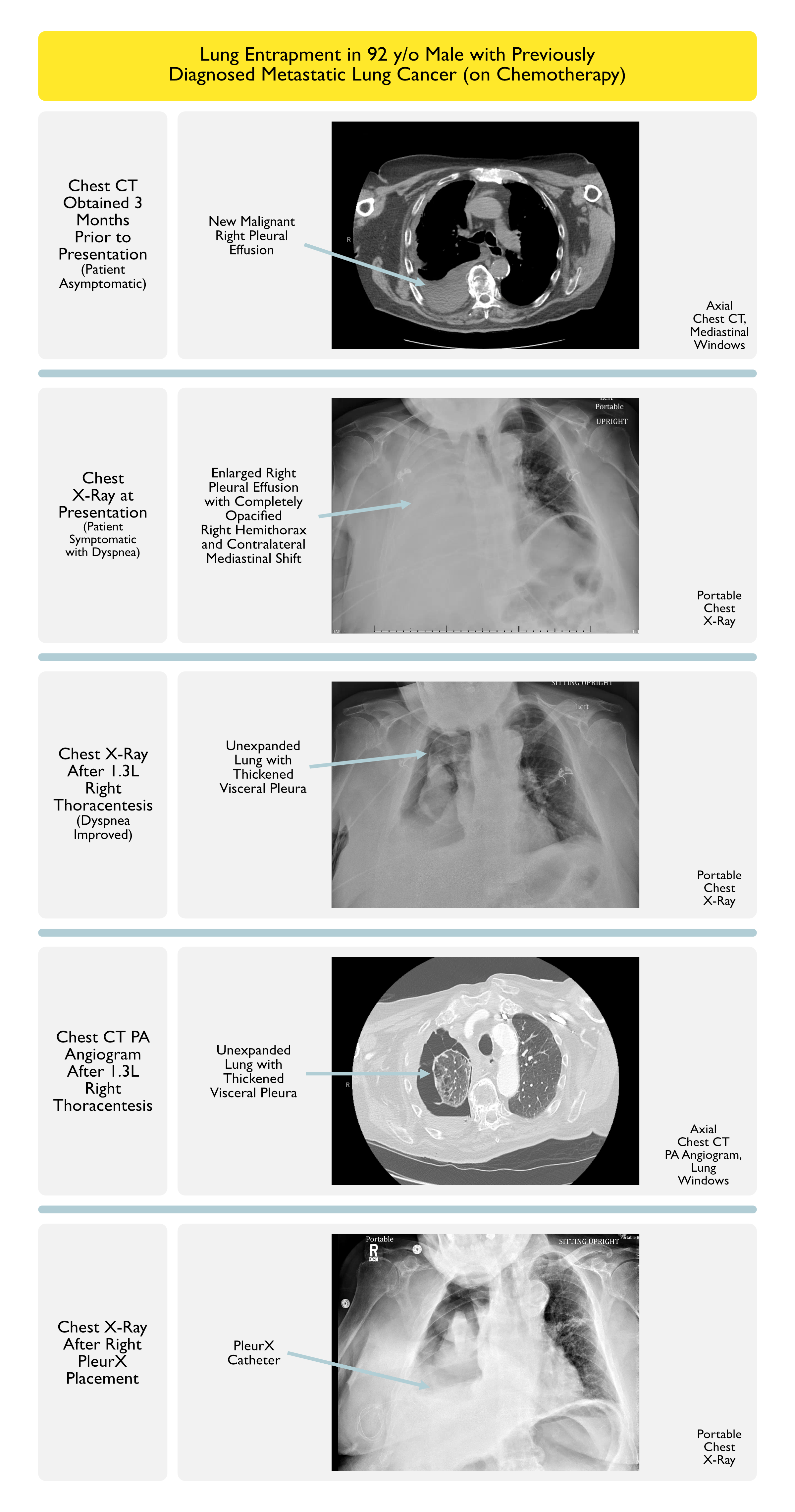
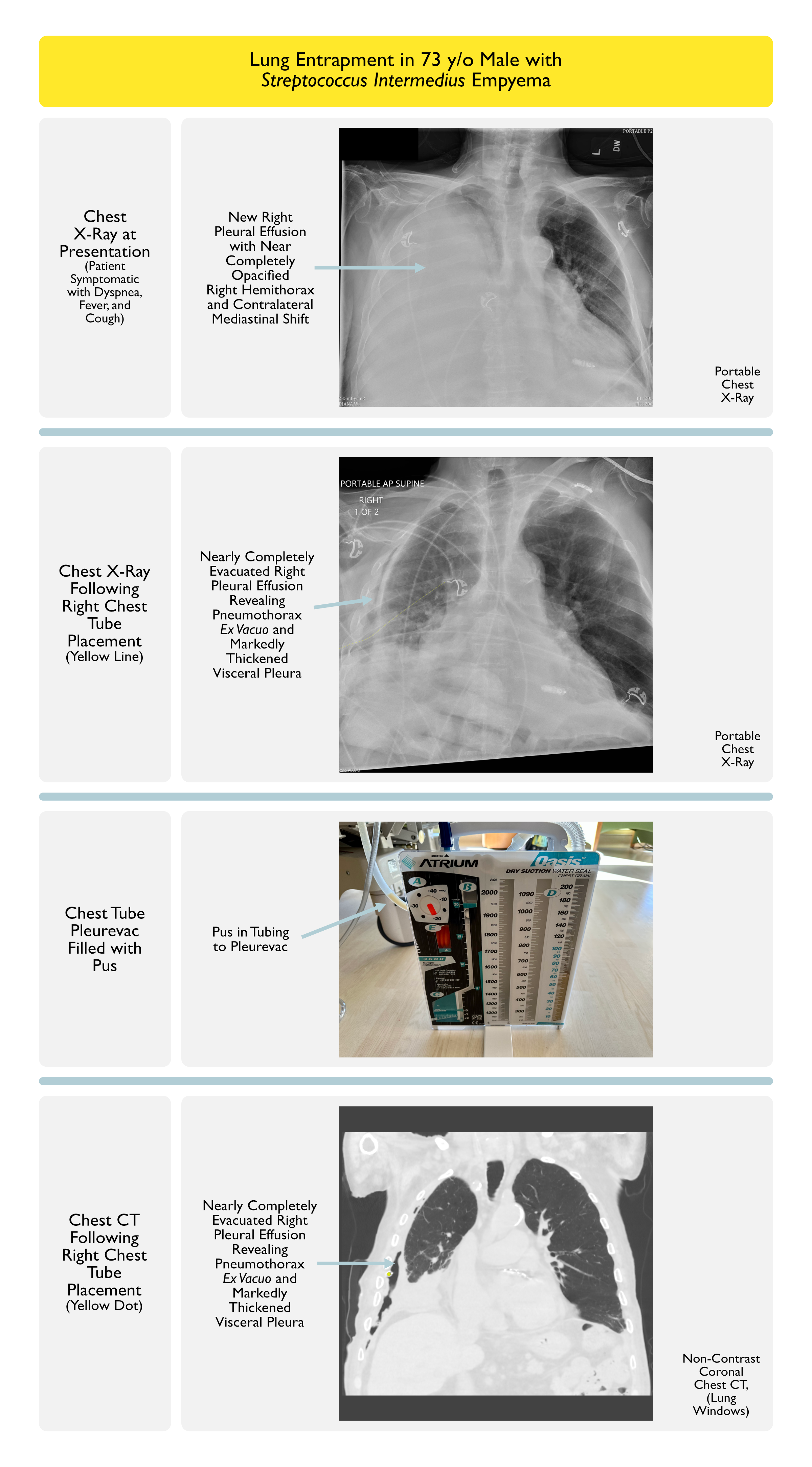
After Thoracentesis with Pleural Fluid Drainage, the Underlying Lung Does Not Fully Expand in a Patient with Lung Entrapment (Creating Pneumothorax Ex Vacuo)
Lack of Lung Expansion at the Base of the Lung is Particularly Indicative of Lung Entrapment
Etiology of Post-Thoracentesis Air in the Pleural Space (Chest, 2006) [MEDLINE]
Puncture of Visceral Pleura (i.e. True Pneumothorax) (see Pneumothorax)
Entry of Air Alongside the Pleural Drainage Catheter Due to Negative Pressure in the Pleural Space (i.e. True Pneumothorax or Pneumothorax Ex Vacuo) (see Pneumothorax)
Small Visceral Pleural Defects Which are Created by Local Deformation Forces in Response to Negative Pleural Pressures Generated When the Lung Cannot Fully Re-Expand (i.e. “Pneumothorax Ex Vacuo” Associated with Lung Entrapment)
Post-Thoracentesis, Visceral Pleural Thickening May Also Be Seen in Patients with Lung Entrapment
Pleural Manometry (Pressure) Findings During Thoracentesis in a Patient with Lung Entrapment
In Normal Patient with Expandable Lung, the Pressure/Volume Curve is Monophasic with a Normal Elastance of ≤14.5 cm H2O/L (F1000 Med Rep, 2010) [MEDLINE]
Elastance = Change in Pleural Pressure Divided by the Volume of Pleural Fluid Removed
In Lung Entrapment, an Abnormal Biphasic Pressure-Volume Curve (with an Inflection Point) is Observed
Initial Normal Pleural Space Elastance ≤14.5 cm H2O/L is Observed
Then, After the Inflection Point, a Subsequent Higher Pleural Space Elastance >14.5 H2O/L is Observed
Increased Pleural Elastance Measured at the End of Thoracentesis When Minimal Pleural Fluid Remains (i.e. “Terminal Elastance”)
Patient May Develop Chest Discomfort During Therapeutic Thoracentesis (Despite Significant Residual Pleural Fluid Remaining) (Chest, 2009) [MEDLINE]
Chest Discomfort May Be Related to Negative Intrapleural Pressure Created by the Removal of Fluid with Inability of the Lung to Expand to Fill the Space
Pleural Fluid Characteristics
Exudative Pleural Fluid (By Both Lactate Dehydrogenase and Total Protein Criteria) (Clin Chest Med, 2006) [MEDLINE]
However, Discordant Lactate Dehydrogenase and Total Protein Exudates Can Occur as the Inflammatory Process is Resolving
Positive Pleural Fluid Cytology (In Cases Where Pleural Malignancy is the Causative Etiology)
Increased Total Nucleated Cell Count (with Either a Neutrophil or Lymphocyte Predominance, Depending Upon the Etiology of the Lung Entrapment)
Lung Entrapment Can Be Diagnosed by the Occurence of a Pneumothorax Ex Vacuo Following Pleural Drainage
With a Large Pleural Effusion (in Which Contralateral Mediastinal Shift Would Normally Be Expected), Mediastinum is Not Shifted or is Shifted Ipsilaterally, Raising the Suspicion of Lung Entrapment
Usually Only Required When the Etiology of Nonexpandable Lung is Unclear or the Patient Has Refractory Clinical Symptoms
Thoracoscopy Involves General Anesthesia with Positive-Pressure Inflation of the Lung Under Direct Visualization
Alternatively, When Performing Medical Thoracoscopy (i.e. Pleuroscopy), Which is Instead Performed Under Negative-Pressure Ventilation, it May Be Difficult to Predict the Existence of Nonexpandable Lung (Respirology, 2016)[MEDLINE]
Clinical
General Comments
Patients with Lung Entrapment May Be Asymptomatic in Some Cases
In Some Patients with Lung Entrapment Due to Pleural Inflammation (Such as Rheumatoid Pleuritis), Pleural Disease Can Be the Initial Presenting Clinical Finding of the Disease (But Findings Related to the Underlying Disease More Commonly Will Be Present)
Treat the Underlying Infection/Inflammation/Malignancy
However, Malignancy-Associated Lung Entrapment Rarely Responds to Chemotherapy (Am J Med Sci, 2008) [MEDLINE]
Periodic Thoracentesis with Pleural Fluid Drainage (see Thoracentesis)
Commonly Used to Improve Dyspnea
Since Pleural Effusion-Associated Dyspnea is Not Related to Lung Collapse (Atelectasis), Hypoxemia, or Loss of FEV1 (But is More Likely a Chest Wall Phenomenon Due to Flattening and Inefficiency of the Length-Tension Relationship of the Diaphragm), Patients with Lung Entrapment May Experience a Significant Decrease in Dyspnea After Thoracentesis Pleural Fluid Drainage Despite a Lack of Lung Expansion (Am J Med, 1983) [MEDLINE]
An Observed Post-Thoracentesis Decrease in Dyspnea Suggests that Strategies to Decrease Pleural Fluid Accumulation Will Be Expected to Provide Continued Symptomatic Relief
Importantly, if a Patient with Malignancy-Associated Pleural Effusion Fails to Experience Symptomatic Relief of Dyspnea Following Therapeutic Thoracentesis, Consideration Should Be Given to Other Potential Etiologies of Dyspnea (Acute Pulmonary Embolism, Airway Obstruction, Deconditioning, Heart Failure, etc)
In Contrast, a Failure to Observe Post-Thoracentesis Decrease in Dyspnea Indicates that Further Measures to Decrease Pleural Fluid Accumulation are Not Necessary
PleurX Catheter is Easily Placed with Local Anesthesia with/without Minimal Moderate Sedation
PleurX Catheter Infection Rate is Low (Chest, 2013) [MEDLINE]
PleurX Catheter Placement is Commonly Used to Manage Malignant Pleural Effusion-Associated Lung Entrapment with Dyspnea Who Exhibit Symptomatic Relief with Pleural Drainage (and for Malignant Pleural Effusion-Associated Dyspnea without Lung Entrapment, as Well) (Ann Intern Med, 1997) [MEDLINE]
PleurX Catheter Allows Intermittent Pleural Fluid Drainage at Home
Approximately 50% of Patients with Malignancy-Associated Nonexpandable Lung Treated with an Intrapleural Catheter (PleurX, etc) Achieve Lung Re-Expansion After 6 Months (Lancet Respir Med, 2018) [MEDLINE]
Note that in Malignant Pleural Effusion-Associated Lung Entrapment with Dyspnea, the Inability of the Lung to Fully Expand and Achieve Pleural Apposition is a Contraindication to Pleurodesis (Ann Intern Med, 1997) [MEDLINE] (see Pleurodesis (see Pleurodesis)
In Such Patients, Pleurodesis Has Been Demonstrated to Frequently Fail in Malignancy-Associated Lung Entrapment Who Exhibit a Decrease in Pleural Pressure >19 cm H2O After the Removal of 500 mL of Pleural Fluid (Ann Intern Med, 1997) [MEDLINE]
Pleuroperitoneal Shunt is Less Used Today Due to its Invasiveness and the Relative Ease of PleurX Catheter Placement
Requires Thoracoscopic Guidance Under General Anesthesia
Because Intraperitoneal Pressure is Typically Higher than the Pleural Space Pressure, the Patient Must Compress the Pump Chamber Multiple Times Per Day to Facilitate Drainage of the Pleural Fluid into the Peritoneal Space
Pleuroperitoneal Shunt-Related Complications (Infection, Occlusion) Occur in Approximately 15% of Cases
Fibrotic Process Involving the Visceral Pleura Prevents Full Lung Expansion (Which is Observed After the Removal of Pleural Fluid)
Negative Pleural Pressure Increases the Entry of Fluid into the Pleural Space and Decreases the Efflux of Fluid Out of the Pleural Space by Pleural Lymphatics
The Resulting Steady State Culminates in Accumulation of a Persistent Negative-Pressure Pleural Effusion of a Remarkably Constant Volume Over Time (Am Rev Respir Dis, 1980) [MEDLINE]
The Persistence of the Pleural Effusion is Mechanical (i.e. Pleural Effusion “Ex Vacuo”) (Semin Respir Crit Care Med, 2001) [MEDLINE]
Thoracentesis Typically Causes Chest Discomfort Throughout the Drainage Procedure (Due to Further Decrease in the Pleural Pressure)
After Thoracentesis with Pleural Fluid Drainage, the Underlying Lung Does Not Fully Expand in a Patient with Trapped Lung (Creating Pneumothorax Ex Vacuo)
Etiology of Post-Thoracentesis Air in the Pleural Space (Chest, 2006) [MEDLINE]
Puncture of Visceral Pleura (i.e. True Pneumothorax) (see Pneumothorax)
Entry of Air Alongside the Pleural Drainage Catheter Due to Negative Pressure in the Pleural Space (i.e. True Pneumothorax or Pneumothorax Ex Vacuo) (see Pneumothorax)
Small Visceral Pleural Defects Which are Created by Local Deformation Forces in Response to Negative Pleural Pressures Generated When the Lung Cannot Fully Re-Expand (i.e. Pneumothorax Ex Vacuo Associated with Trapped Lung)
Pleural Manometry (Pressure) Findings During Thoracentesis in a Patient with Trapped Lung
In Normal Patient with Expandable Lung, the Pressure/Volume Curve is Monophasic with a Normal Elastance of ≤14.5 cm H2O/L (F1000 Med Rep, 2010) [MEDLINE]
Elastance = Change in Pleural Pressure Divided by the Volume of Pleural Fluid Removed
In Trapped Lung, Initial Pleural Pressure is Usually Slightly Negative and the Pleural Pressure Decreases Quickly as Pleural Fluid is Removed (Monophasic Curve with Pleural Space Elastance is >14.5 cm H2O/L)
In Patients with More than One Etiology of Their Pleural Effusion, Pleural Manometry May Be Complicated, Since a Patient May Have Initial Normal Pleural Elastance (For Example, Due to Partial Lung Re-Expansion Associated with the Removal of the Hydrostatic Component of Fluid in a Heart Failure Patient), with a Terminal Elastance Being Abnormally High (Due to the Remaining Nonexpandable Lung)
Pleural Fluid Characteristics
By Lactate Dehydrogenase (LDH) Criteria, Pleural Fluid is Either Transudative or Borderline Exudative
By Total Protein Criteria, Pleural Fluid is Either Transudative or Exudative
Pleural White Blood Cell Count is Predominantly Mononuclear
Fluid May Shift Somewhat with Changes in Body Position, But is Not Free-Flowing
Paradoxically, Hemithorax with the Pleural Effusion is Decreased in Size as Compared to the Contralateral Side
Due to Pleural Pressure on the Affected Side Being More Negative than on the Contralateral Side
Air Contrast Chest CT
While Controversial, the Injection of 200-400 mL of Air into Pleural Space at Conclusion of a Therapeutic Thoracentesis May Accentuate Visualization of the Pleural Rind (Particularly Rinds <3 mm) on Chest CT
This Will Also Increase the Pleural Pressure, Decreasing Patient’s Chest Discomfort
Caution Should Be Given to Avoid Air Travel and Scuba Diving Until the Injected Pleural Air is Reabsorbed
Usually Only Required When the Etiology of Nonexpandable Lung is Unclear or the Patient Has Refractory Clinical Symptoms
Thoracoscopy Involves General Anesthesia with Positive-Pressure Inflation of the Lung Under Direct Visualization
Alternatively, When Performing Medical Thoracoscopy (i.e. Pleuroscopy), Which is Instead Performed Under Negative-Pressure Ventilation, it May Be Difficult to Predict the Existence of Nonexpandable Lung (Respirology, 2016)[MEDLINE]
Clinical
Stable, Chronic Pleural Effusion
Characteristic Clinical Finding
Most Patients are Asymptomatic (i.e. Pleural Effusion is Diagnosed Incidentally on Physical Exam or Chest Imaging)
Limited Case Series Have Demonstrated Efficacy in Patients with Coronary Artery Bypass Graft-Associated Trapped lung (Chest, 2001) [MEDLINE]
References
Observations on pleural fluid pressures as fluid is withdrawn during thoracentesis. Am Rev Respir Dis. 1980;121(5):799 [MEDLINE]
Mechanism of relief of dyspnea after thoracocentesis in patients with large pleural effusions. Am J Med. 1983 May;74(5):813-9 [MEDLINE]
The relationship between pleural pressures and changes in pulmonary function after therapeutic thoracentesis. Am Rev Respir Dis 1986, 133:658-61 [MEDLINE]
Trapped-lung syndrome after cardiac surgery: a potentially preventable complication of pleural injury. Heart Lung. 1990;19(6):671 [MEDLINE]
Management of recurrent malignant pleural effusions. The complementary role talc pleurodesis and pleuroperitoneal shunting. Cancer. 1995;75(3):801 [MEDLINE]
Lung cancer and ipsilateral pleural effusion. Ann Oncol. 1995;6 Suppl 3:S25 [MEDLINE]
Intrapleural talc for the treatment of malignant pleural effusions secondary to breast cancer. Cancer. 1995;75(11):2688 [MEDLINE]
Elastance of the pleural space: a predictor for the outcome of pleurodesis in patients with malignant pleural effusion. Ann Intern Med. 1997;126(10):768 [MEDLINE]
Measurement of pleural pressure during therapeutic thoracentesis. Am J Respir Crit Care Med 2000, 162:1534-8 [MEDLINE]
Characteristics of trapped lung: pleural fluid analysis, manometry, and air-contrast chest CT. Chest. 2007;131(1):206 [MEDLINE]
Therapeutic thoracentesis: the role of ultrasound and pleural manometry. Curr Opin Pulm Med 2007, 13:312-8 [MEDLINE]
Clinical implications of unexpandable lung due to pleural disease. Am J Med Sci. 2008;335(1):21 [MEDLINE]
Assessment of pleural pressure in the evaluation of pleural effusions. Chest. 2009;135(1):201 [MEDLINE]
Thoracic ultrasound in the diagnosis of malignant pleural effusion. Thorax. 2009;64(2):139 [MEDLINE]
The unexpandable lung. F1000 Med Rep. 2010;2:77 [MEDLINE]
Clinical outcomes of indwelling pleural catheter-related pleural infections: an international multicenter study. Chest. 2013 Nov;144(5):1597-602 [MEDLINE]
Medical thoracoscopy: Survey of current practice-How successful are medical thoracoscopists at predicting malignancy? Respirology. 2016;21(5):958 [MEDLINE]
Aggressive versus symptom-guided drainage of malignant pleural effusion via indwelling pleural catheters (AMPLE-2): an open-label randomised trial. Lancet Respir Med. 2018;6(9):671 [MEDLINE]