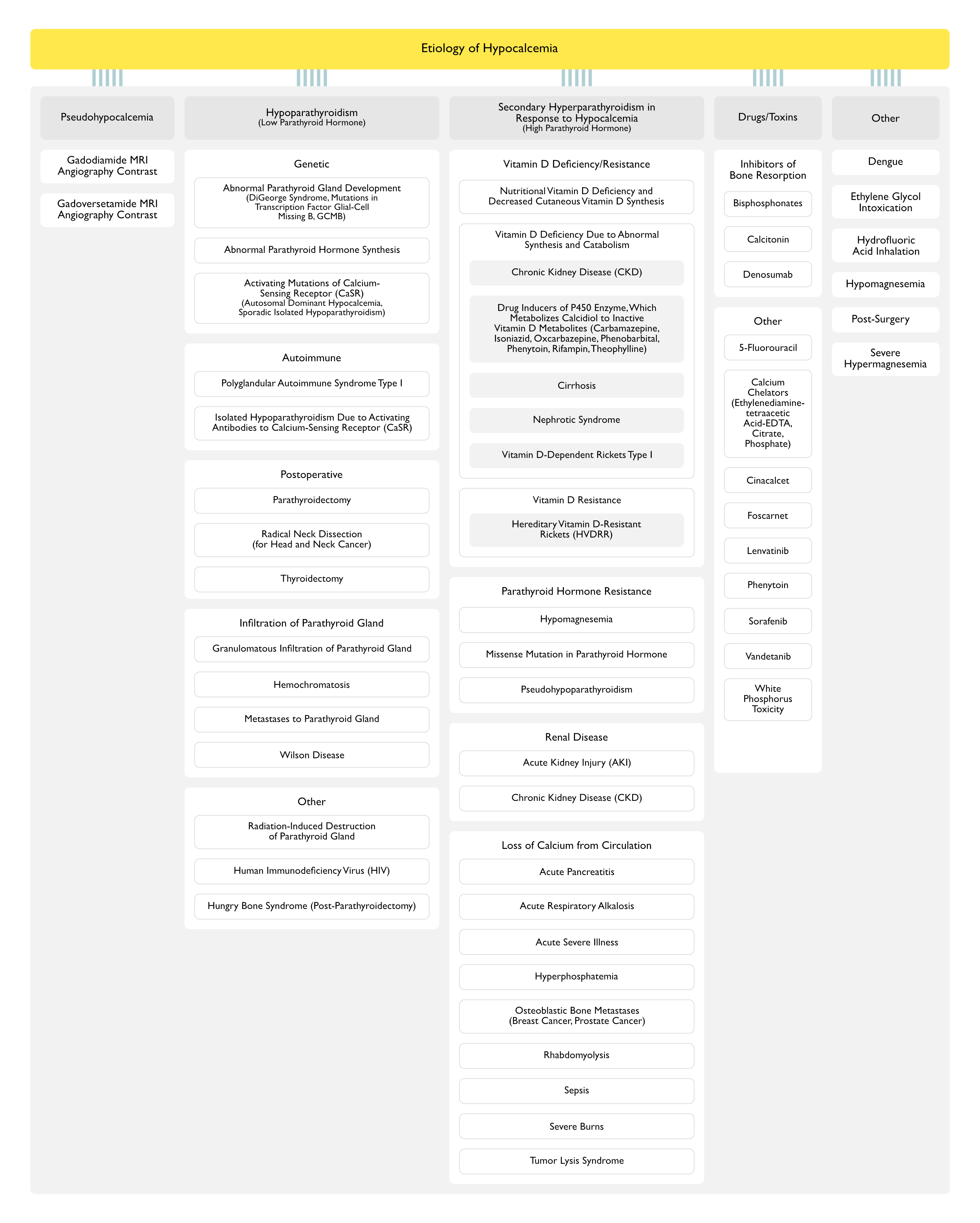
Nutritional Vitamin D Deficiency and Decreased Cutaneous Vitamin D Synthesis
Vitamin D Deficiency Due to Abnormal Synthesis and Catabolism
Chronic Kidney Disease (CKD)
Low Calcitriol (1,25 Dihydroxyvitamin D) Production Due to Decreased Glomerular Filtration Rate, Loss of the 1-Alpha-Hydroxylase Enzyme Secondary to Structural Renal Disease, and Suppression of Enzyme Activity Due to Hyperphosphatemia and Resultant Increased Circulating FGF23 Levels
Drugs (Inducers of P-450 Enzyme, Which Metabolizes Calcidiol to Inactive Vitamin D Metabolites)
Acute Hyperphosphatemia, Resulting from Increased Phosphate Intake (Phosphate Enemas, Oral Phosphate Replacement) in the Setting of Renal Failure, Can Result in Acute Hypocalcemia
Chronic Hyperphosphatemia is Usually Due to Decreased Phosphate Clearance in Chronic Kidney Disease
In These Cases, Primary Impairment of Calcitriol Synthesis (Resulting in Decreased Intestinal Calcium Absorption) Further Exacerbates the Hypocalcemia
Physiology
Hyperphosphatemia Results in Calcium Deposition, Mostly in Bone (But Also in Extraskeletal Tissues)
Patients are Typically Hypocalcemic During the Oliguric Phase of Acute Kidney Injury (Due to Acute Tubular Necrosis)
Physiology
In Setting of Decreased Renal Excretion of Phosphate, Hyperphosphatemia from Tissue Breakdown Results in Calcium Deposition, Mostly in Bone (But Also in Extraskeletal Tissues)
In the Setting of Decreased Renal Excretion of Phosphate, Hyperphosphatemia from Tumor Breakdown Results in Calcium Deposition, Mostly in Bone (But Also in Extraskeletal Tissues)
Hypocalcemia is More Frequently Seen When Potent Bisphosphonates (Such as Zoledronate) are Used and in Patients with Underlying Vitamin D Deficiency, Unrecognized Hypoparathyroidism, or Chronic Kidney Disease
Pharmacology
Bisphosphonates Reduce Osteoclastic Bone Resorption
Denosumab is a Fully Human Monoclonal Antibody to the Receptor Activator of Nuclear Factor Kappa B Ligand (RANKL), Which is an Osteoclast Differentiating Factor
Other Drugs/Toxins
5-Fluorouracil (5-FU) and Leucovorin (see 5-Fluorouracil)
Epidemiology
Hypocalcemia Occurred in 65% of Cases (in One Series of Patients)
Physiology
Probably Due to a Decrease in Calcitriol Production
Dengue Fever Has Been Associated with Hypocalcemia (Int J Crit Illn Inj Sci, 2014) [MEDLINE]
Physiology
Likely Multifactorial
Clinical
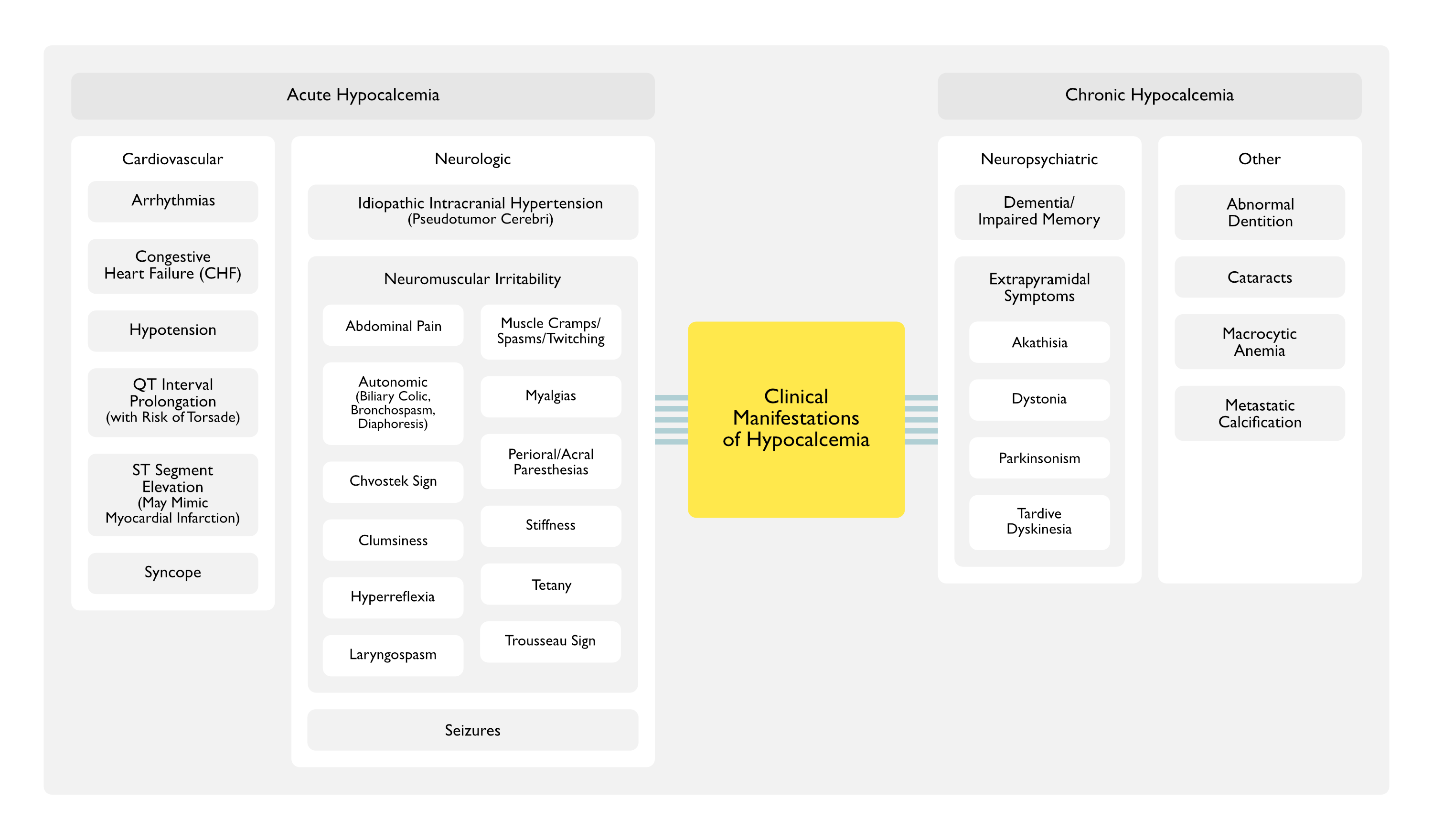
As Suggested in In Vitro Studies, Derangements of Calcium Homeostasis are Likely to Be Associated with Myocardial Dysfunction and Cardiac Arrhythmias in the Setting of Dengue Virus Infection
Cases of Hypocalcemia-Associated Hypotension Have Been Extensively Reported (Am J Kidney Dis, 1994) [MEDLINE] (Am J Kidney Dis, 2015) [MEDLINE] (Hemodial Int, 2016) [MEDLINE]
Hypocalcemia-Associated Hypotension is Most Commonly Seen When it is Rapidly Induced by Ethylenediaminetetraacetic Acid (EDTA), Transfusion of Citrated Blood, Products, or with the Use of Low Calcium Dialysate in Patients Undergoing Dialysis
Physiology
XXXX
Prolonged Q-T with Increased Risk of Torsade (see Torsade)
Patients with a Gradual Decline in Serum Calcium Tend to Have Fewer Symptoms at the Same Calcium Level than Patients with Acute Hypocalcemia (Endocrinol Metab Clin North Am, 1993) [MEDLINE]
Tetany Usually Only Occurs when Ionized Calcium Falls to Below 1.1 mmol/L (Corresponding to a Total Serum Calcium of Approximately 7-7.5 mg/dL)
Physiology
Acute Hypocalcemia Increases Neuromuscular Irritability (Brain, 1991) [MEDLINE]: hyperexcitability occurs at central nervous system level, spinal reflex level, and motor endplate level
Other Name for Sign: “main d’accoucheur” (French for “hand of the obstetrician”) because it resembles the position of an obstetrician’s hand in delivering a baby
Inflated Blood Pressure Cuff for 3 min Elicits Carpopedal Spasm in the Hand/Forearm
Systematic Review of Parenteral Calcium Replacement in Critical Care Patients (Cochrane Database Syst Rev, 2008) [MEDLINE]: no evidence that parenteral calcium replacement improves outcome in critically ill patients
Agents
Calcium Chloride (in 10 ml = 10%) (see Calcium Chloride): 1 amp over 30-60 min
Massive blood replacement: correlation of ionized calcium, citrate, and hydrogen ion concentration. Anesth Analg 1979; 58:274-278 [MEDLINE]
Paraesthesiae and tetany induced by voluntary hyperventilation. Increased excitability of human cutaneous and motor axons. Brain. 1991;114 ( Pt 1B):527 [MEDLINE]
Hypocalcemic emergencies. Endocrinol Metab Clin North Am. 1993;22(2):363 [MEDLINE]
Ionized hypocalcemia during sepsis. Crit Care Med 2000; 28:266-268 [MEDLINE]
Electrolyte disturbances in the intensive care unit. Semin Dial 2006; 19:496-501 [MEDLINE]
Parenteral calcium for intensive care unit patients. Cochrane Database Syst Rev 2008 Oct 8; (4):CD006163. DOI: 1002/14651858.CD006163.pub2 [MEDLINE]
Calcium homeostasis during magnesium treatment in aneurysmal subarachnoid hemorrhage. Neurocrit Care 2008;8(3):413 [MEDLINE]
Hypocalcaemia in an adult: the importance of not overlooking the cause. BMJ Case Rep. 2018 Apr 5;2018. pii: bcr-2017-224108. doi: 10.1136/bcr-2017-224108 [MEDLINE]
Clinical Presentation of Hypoparathyroidism. Front Horm Res. 2019;51:139-146. doi: 10.1159/000491044 [MEDLINE]
Other
Cardiac failure associated with hypocalcemia. Anesth Analg. 1976;55(1):34 [MEDLINE]
Hypocalcemic heart failure in end-stage renal disease. Am J Nephrol 1990;10(2):167-70. doi: 10.1159/000168073 [MEDLINE]
Hypocalcemic emergencies. Endocrinol Metab Clin North Am. 1993;22(2):363 [MEDLINE]
Refractory hypotension associated with hypocalcemia and renal disease. Am J Kidney Dis 1994 Mar;23(3):430-2. doi: 10.1016/s0272-6386(12)81007-9 [MEDLINE]
Reversible hypocalcemic heart failure with T wave alternans and increased QTc dispersion in a patient with chronic renal failure after parathyroidectomy. Clin Nephrol 2006 Jan;65(1):65-70. doi: 10.5414/cnp65065 [MEDLINE]
Reversible congestive heart failure related to profound hypocalcemia secondary to hypoparathyroidism. Am J Med Sci 2007 Apr;333(4):226-9. doi: 10.1097/MAJ.0b013e318039b9c6 [MEDLINE]
Facility Dialysate Calcium Practices and Clinical Outcomes Among Patients Receiving Hemodialysis: A Retrospective Observational Study. Am J Kidney Dis. 2015 Oct;66(4):655-65 [MEDLINE]
Dialysate-induced hypocalcemia presenting as acute intradialytic hypotension: A case report, safety review, and recommendations. Hemodial Int. 2016;20(2):E8 [MEDLINE]
Treatment
Choice of calcium salt. A comparison of the effects of calcium chloride and gluconate on plasma ionized calcium. Anaesthesia. 1984 Nov;39(11):1079-82 [MEDLINE]
Calcium chloride versus calcium gluconate: comparison of ionization and cardiovascular effects in children and dogs. Anesthesiology. 1987 Apr;66(4):465-70 [MEDLINE]
Ionization and hemodynamic effects of calcium chloride and calcium gluconate in the absence of hepatic function. Anesthesiology. 1990 Jul;73(1):62-5 [MEDLINE]