Conus Medullaris: the spinal cord tapers and ends between L1 and L2, with the conus medullaris representing the most distal bulbous part of the spinal cord
Blood Supply
Spinal arteries (anterior median longitudinal arterial trunk and 2 posterolateral trunks): main supply
Radicular Arterial Branches from Aorta: less prominent arterial supply
Lateral Sacral Artery: less prominent arterial supply
Fifth Lumbar Artery: less prominent arterial supply
Iliolumbar Artery: less prominent arterial supply
Middle Sacral Artery: less prominent arterial supply
Cauda Equina (“horse tail”): mass of lower lumbar and S1-S5 nerve roots distal to the conus medullaris (and within the subarachnoid space)
Sensory Innervation: to the saddle area (perineal dermatomes) and lower extremity dermatomes
S2-S4 -> pudendal nerve -> voluntary muscles of urethral sphincter
Lower extremity myotomes
Parasympathetic Innervation: to the bladder and lower part of the colon (from splenic flexure to the rectum)
S2-S4 -> pelvic splanchnic nerves -> detrusor muscle of bladder
Compression of the cauda equina technically represents a “peripheral” nerve injury
Blood Supply: middle sacral artery
Filum Terminale: the fibrous (non-neural) extension of the spinal cord, which extends down to the coccyx
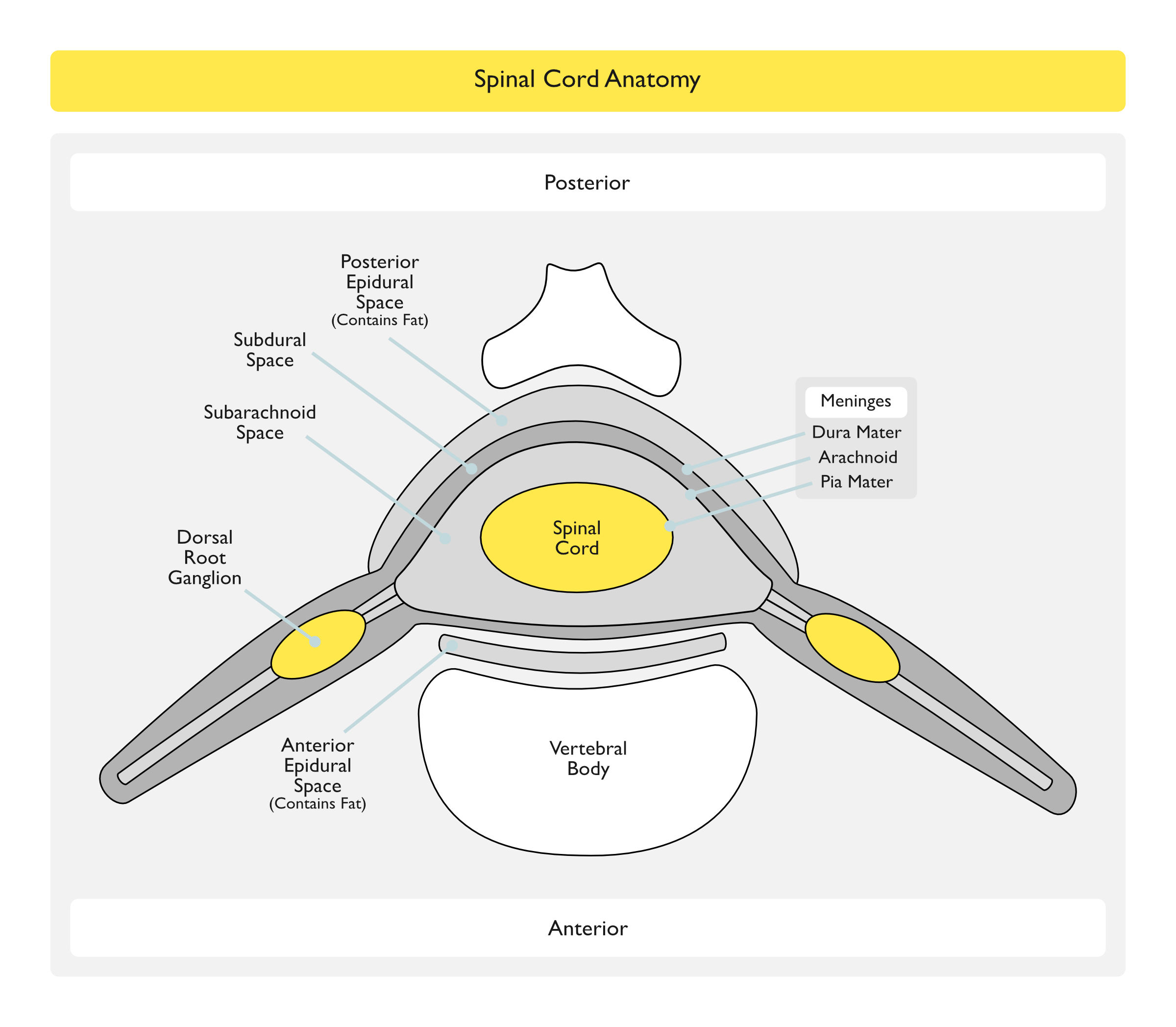
Epidural Space
Posterolateral Epidural Space
Anatomy
Posterolateral epidural space extends vertically down the spinal canal and contains arteries, venous plexus, and fat
Posterolateral epidural space is larger than the anterior epidural space
Posterolateral epidural space is larger in the sacral region than it is in the cervical region
Posterolateral Epidural Abscess
Posterior epidural abscess is more common than anterior epidural abscess, due to larger size of the posterior epidural space (with more infection-prone fat) and a more extensive venous plexus (which allows microbiologic seeding of the space)
Thoracolumbar posterior epidural abscess is the most common location in the spine, due to larger size of the epidural space (with more infection-prone fat)
Vertical extension of abscess commonly occurs: average extent of extenson is 3-5 spinal cord segments (although some cases manifest pan-spinal infection)
Lumbar epidural abcsess is predisposed by the use of epidural procedures for pain management
Anterior Epidural Space
Anatomy
Anterior epidural space is a virtual space under normal circumstances (due to adherence of dura to bone of vertebral bodies from the foramen magnum down to L1)
Anterior Epidural Abscess
Anterior spinal epidural abscess usually occurs below L1 (due to adherence of dura to bone of vertebral bodies from the foramen magnum down to L1)
Anterior spinal epidural abscess is usually associated with vertebral osteomyelitis
Etiology
Bacteremia with Hematogenous Spread to Epidural Space (approximately 50% of cases)
The location of spinal epidural abscess is correlated with the sites of injection: cervical spinal epidural abscess is more common in those with upper extremity injection sites, while lumbar spinal epidural abscess is more common in those with lower extremity injection sites
Contiguous Spread to Epidural Space (approximately 33% of cases)
Direct Inoculation Into Epidural Space
Epidural Anesthesia: 0.5-3% of cases are complicated by spinal epidural abscess
Short-term epidural catheter use (as in obstetrical cases) is associated with significantly decreased risk (study cited only one case in 506k obstetric epidural cases)
Epidural space infection can occur via multiple possible mechanisms: infection at time of catheter placement, ascending contamination from skin flora, contaminated syringes or injected solutions, or from bacteremic seeding while catheter is in place
21-40% of Staphylococcus Aureus cases are methicillin-resistant Staphylococcus aureus (MRSA): the incidence of MRSA and MRSA-epidural abscess cases has increased in the past decade
MRSA is partcularly common in patients with spinal or other implantable devices
Spinal epidural abscess outcomes are worse with MRSA than with non-MRSA Staphylococcus aureus
Gram-Negative Rods: 16% of cases
Escherichia Coli (see Escherichia Coli): associated with urinary tract infection (UTI)
Radionuclide Scanning (technetium, gallium, indium): although these may demonstrate increased uptake, they have high false-negative rates
Epidural Abscess Cultures: positive in 90% of cases
Lumbar Puncture/CSF: lumbar puncture (that might be performed to rule out meningitis/encephalitis) should be performed only after after spine MRI rules out the presence of an epidural collection that might be traversed by the needle (due to the risk of disseminatng the infection) [MEDLINE]
Lumbar puncture can also result in neurologic deterioration if if is perfomed below the site of a complete spinal subarachnoid block
CSF Gram Stain: almost always negative
CSF Cultures: positive in <25% of cases
Blood cultures are usually positive in cases with positive CSF cultures
CSF Cell Count: pleocytosis may be seen (either polymorphonculear or mononuclear-predominance)
CSF Protein: non-specific elevation may be seen
Clinical Manifestations
Classical Triad of Clinical Symptoms/Signs
General Comments: classical triad is uncommon at initial presentation
Diagnostic Guidelines for Evaluation of Back Pain in the Emergency Department: evaluation with risk factor assessment and CRP/ESR testing prior to imaging has been shown to decrease diagnostic delay and decrease motor deficits at the time of diagnosis in spinal epidural abscess [MEDLINE]
Chest Pain (see Chest Pain): may occur in thoracic spine epidural abscess
Neck Pain (see Neck Pain): commonly occurs in cervical epidural abscess
Root Pain: with character of “shooting” or “electric shocks” in distribution of the affected nerve root, may appear later
Neurologic Symptoms (33% of cases): typically these are late findings
Cauda Equina Syndrome (see Cauda Equina Syndrome): for cases with involvement of cauda equina (cauda equina is the mass of lower lumbar and S1-S5 nerve roots distal to the conus medullaris)
Areflexia
Ankle
Bladder/Bowel Dysfunction
Decreased Anal Tone/Fecal Incontinence
Urinary Retention: due to detrusor muscle weakness
Urinary Incontinence
Low Back Pain/Sciatica: sciatica may be unilateral or bilateral
Pneumonia (see Pneumonia): in cases with cervical epidural abscess
Treatment
Neurosurgical Drainage/Evacuation of Inflammatory Tissue
Therapeutic Procedure of Choice: surgical evacuation is considered the standard of care to both relieve the cord compression and control sepsis
Predictors of Neurologic Outcome: extent and duration of neurologic deficit prior to surgery
Possible Contraindications to Surgery: while a non-surgical strategy can be used in very select patients (for example: those without neurologic defiicts), it requires close monitoring for potential neurologic deterioration (allowing for prompt surgical intervention at that point in time)
Patient Refusal to Undergo Surgery
Medical Contraindications to Surgery
Presence of Advanced Neurologic Deficits Which are Unlikely to Improve with Surgery: complete paralysis >24-48 hrs duration
Large Extent of Spinal Involvement/Panspinal Involvement: which may make surgery impractical (although in these cases, a limited surgical exposure with cranial/caudal placement of epidural catheters may be utilized)
Absence of Neurologic Deficits
Timing of Surgery:: surgery should be performed as soon as possible (generally within 24-36 hrs)
Rate of progression is unpredictable
Paralysis present for >24 hrs is unlikely to improve with surgical decompression
Therapeutic Needle Aspiration of Epidural Abscess
May be considered in select cases without evidence of cord compression
Antibiotics
Length of Treatment: prolonged course with IV antibiotics is required (usually 6-8 weeks or until resolution of abscess on MRI)
Empiric Therapy: Vancomycin IV + Metronidazole IV + Ceftriazone/Cefotaxime/Ceftazidime IV
Targeted Therapy: guided by blood cultures, needle aspiration of abscess, or surgical cultures
May be used in select cases to decrease spinal edema in cases with progressive neurologic compromise pre-operatively
Post-Acute Care
Follow-Up Spine MRI: usully indicated at about 4 wks into therapy (or earlier, if neurologic deterioration occurs)
Spinal Cord Rehabilitation: may lead to moderate-marked improvement in motor function in some cases, even up to a year later
Prognosis:
Mortality Rate: 5% (usually due to sepsis, uncontrolled meningitis, or other underlying co-morbid illness)
Recurrence of Epidural Abscess: may occur in successfully-treated cases who are subsequently treated with immunosuppressives (glucocorticoids, etc) or later become immunocompromised
References
General
Decreased morbidity from acute bacterial spinal epidural abscesses using computed tomography and nonsurgical treatment in selected patients. Ann Neurol 1985, 17:350–355 [MEDLINE]
Spinal epidural abscess. N Engl J Med 2006; 355: 2012-20 [MEDLINE]
Spinal epidural abscess in clinical practice. Q J Med 2008; 101: 1–12 [MEDLINE]
Management of a spontaneous spinal epidural abscess: a single-center 10-year experience. Neurosurgery 2009, 65:919–923; discussion 923–914 [MEDLINE]
Spinal epidural abscess. J Emerg Med 2010; 39(3): 384–390 [MEDLINE]
Spinal epidural abscess: Current Diagnosis and Management. Curr Infect Dis Rep 2010; 12: 484-491 [MEDLINE]
Prospective evaluation of a clinical decision guideline to diagnose spinal epidural abscess in patients who present to the emergency department with spine pain. J Neurosurg Spine. 2011 Jun;14(6):765-70 [MEDLINE]
Epidemiology
Spinal epidural abscess: a review of epidemiology, diagnosis, and treatment. J Spinal Disord 1999, 12:89–93 [MEDLINE]
Nocardial epidural abscess of the thoracic spinal cord and review of the literature. J Infect Chemother. 2005;11(3):169 [MEDLINE]
Nocardial spinal epidural abscess with lumbar disc herniation: A case report and review of literature. Medicine (Baltimore). 2018;97(49):e13541 [MEDLINE]
Disseminated Nocardia farcinica infection presenting as a paravertebral abscess in a patient with systemic lupus erythematosus. Indian J Pathol Microbiol. 2019;62(2):329 [MEDLINE]
Diagnosis
Spinal epidural abscess: a review of epidemiology, diagnosis, and treatment. J Spinal Disord 1999, 12:89–93 [MEDLINE]
Treatment
Spinal epidural abscess: a review of epidemiology, diagnosis, and treatment. J Spinal Disord 1999, 12:89–93 [MEDLINE]
A retrospective study of surgical and conservative treatment for spinal extradural abscess. Eur Spine J 2000, 9:67–71 [MEDLINE]